The Consistency Curve: Why Month 3 Is When Clients Quit

Your Tuesday Morning Roster Is Already Telling You Who Will Quit
It is a Tuesday morning. Sam logs into her coaching app at 6:43 a.m. before her first in-person session. Five clients have check-ins due. The first three she handles quickly: workouts logged, sleep okay, weight stable. The fourth is empty. Margaret has not logged a session in eight days. The fifth is the message every online coach has read a hundred times: "Hey Sam, I've been so busy this week. Let me get back on track next week and we'll catch up Monday. Sorry for the radio silence!"
That is the standard goodbye prefix. Sam has seen it before. Both clients started in January and are now at Day 73 and Day 81 respectively. Neither will be on the roster by the end of June.
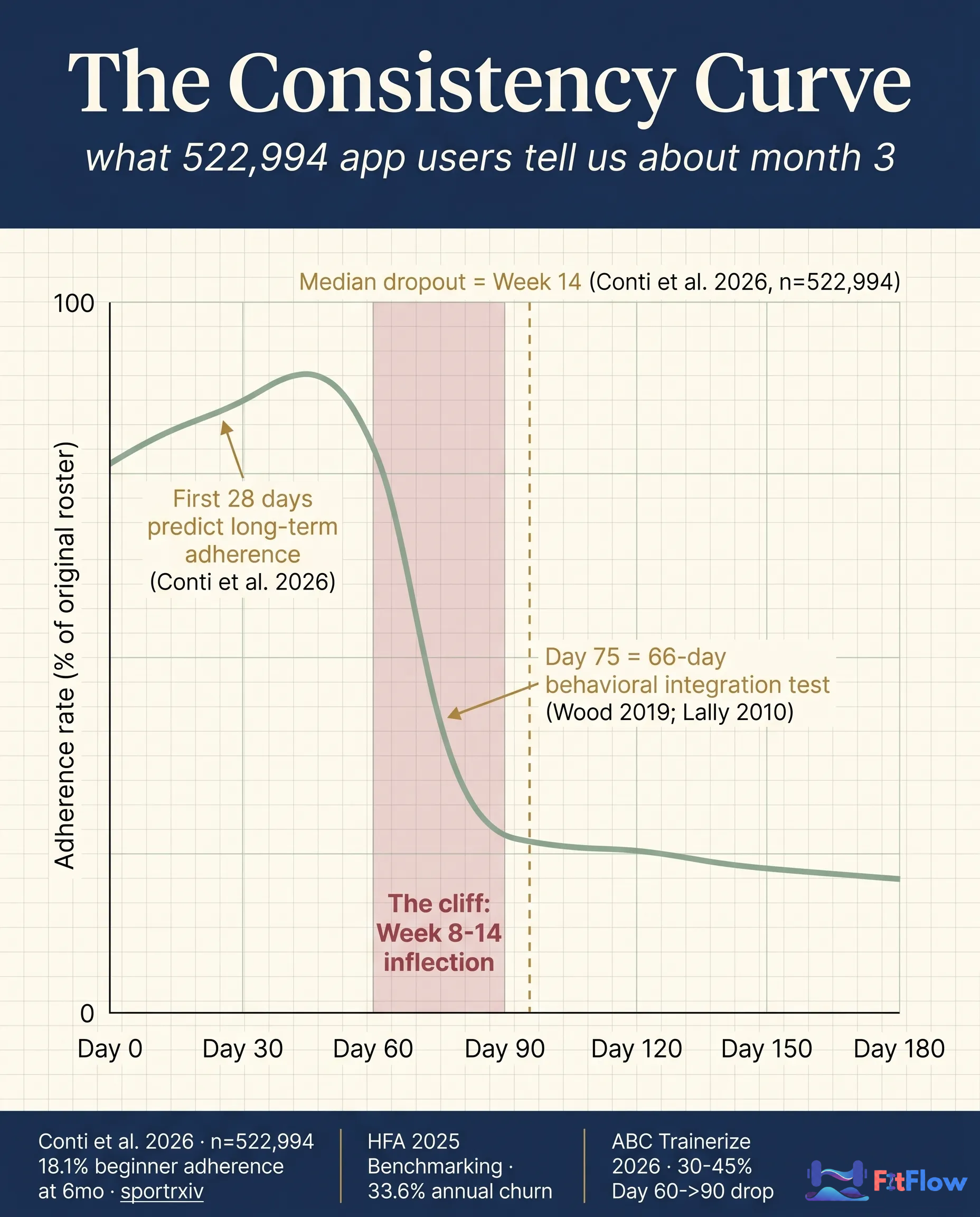
Every coach with a roster bigger than ten clients sees this pattern. Clients fall off in a predictable window, somewhere between Week 8 and Week 14, with the cluster centering on Day 60 to Day 90. The largest cohort study in the field (Conti, Marzagao, Galpin, and Schoenfeld 2026 (preprint), tracking 522,994 adult mobile app users) places median dropout at Week 14 and 6-month adherence at 18.1% for beginners. Roughly 30-45% of online-coached clients drop off between Day 60 and Day 90, per the ABC Trainerize 2026 platform-level dataset. The industry has a name for what comes next: re-engagement campaigns, win-back emails, return discounts. What it has never named is the shape that produces the pattern in the first place.
Call it the consistency curve. It rises through Months 1 and 2, then dips sharply at the Month-3 inflection. The dip is not random. It is not "clients lost motivation." The dip is what happens when the program you wrote on Day 1 is biologically wrong for the body your client has on Day 75, and you, the coach, did not pivot.
Month 3 looks like a motivation problem and acts like a dose-response problem. The original training stimulus has accommodated. The client's body is no longer responding to the program that produced gains in Weeks 1-6. Behavioral fatigue arrives because the underlying biology stopped producing the validating feedback (gains, performance, body-comp change) that powered the first 60 days of consistency. Coaches who fix retention with check-in cadence, gamification, and accountability nudges are solving the wrong layer. The actual fix is a periodization decision the coach failed to make on Week 8.
Get the diagnostic instrument while you read. Download "The Month-3 Churn Audit", a roster-level scoring tool that maps every at-risk client (Day 50-90) to one of four pivot recommendations in under 20 minutes. Built for coaches managing 20-50+ clients. Get the free Audit →
This article delivers the curve in data from 522,994 app users, the dollar cost per Month-3 churn, the four physiological transitions of Week 8-12, the 4-Layer Diagnostic Framework, the Week-8 Programming Pivot Map (sets, reps, intensity, client scripts, 4-week arcs), a two-client case study, platform integration notes, and population variants. Hold the thesis as you read: programming first, behavior second.
The consistency curve is the predictable shape of client adherence over time in personal training. It rises through Months 1-2 (novelty adherence high, dose-response strong), then dips sharply at Weeks 8-12 (Month 3), as the original training stimulus stops producing adaptation and the client's behavioral routine encounters its first true integration test. The dip is not a motivation event. It is a dose-response event.
The Curve Itself: What the Data Actually Shows
The Month-3 inflection is not anecdotal. Three independent 2025-2026 data sources point at the same window. They use different methodologies, different population sizes, and different definitions of "retention." They land in the same Week 8-14 cluster.
The Headline Stat: Conti et al. 2026 preprint (Galpin and Schoenfeld, Co-Authors)
Conti, Marzagao, Galpin, and Schoenfeld 2026 (preprint) tracked 522,994 adult mobile app users for resistance training adherence. Median dropout: Week 14 (Month 3.5). 6-month adherence rate for beginners: 18.1%. Strongest predictor of long-term adherence: training consistency in the first 28 days [Conti et al., 2026 (preprint), sportRxiv].
Half a million users is the largest known adherence sample for resistance training, co-authored by Andrew Galpin and Brad Schoenfeld. The preprint published January 27, 2026; no top-10 page in the personal-training-retention SERP has cited it as of this writing.
The Industry Benchmark and the Platform Cliff
The Health & Fitness Association (formerly IHRSA) 2025 Benchmarking Report tracked 17,000+ facilities. Annual retention: 66.4%. Annual churn: 33.6%. Industry retention has declined ~5 percentage points from 2015 [HFA, 2025]. Distributed across a fitness-specific monthly distribution, the churn concentrates at Months 2-4.
ABC Trainerize 2026 State of the Personal Training Industry Report confirms the platform-level cliff: a 30-45% drop from Day 60 to Day 90 across the Trainerize-coached client base [ABC Trainerize, 2026]. The same report named "retention is the new growth strategy." Three independent sources, three methodologies, one converging window.
Retention by Segment
The single-number "average retention" reading hides the pattern. Segmented, the inflection is more legible:
Segment | Month-3 Retention Picture | Source |
|---|---|---|
Resistance-training app users (beginners) | 18.1% at 6 months; median dropout Week 14 | Conti et al. 2026 (preprint), n=522,994 |
Industry-wide gym/PT facilities | 66.4% annual retention; Month 2-4 concentrated | HFA 2025 Benchmarking |
Online coaches (Trainerize-platform) | 30-45% drop Day 60 → Day 90 | ABC Trainerize 2026 |
Average PT client tenure | 3-6 months; <15% reach 50 sessions | Institute of Personal Trainers 2026 |
Novice (<12 months training) | Highest Month-3 risk | Conti et al. 2026 (preprint) + practitioner consensus |
Intermediate hypertrophy (12-24 mo) | Canonical Month-3 dip; classic accumulation accommodation | Schoenfeld et al. 2017+ |
Paid-monthly | Higher Month-3 risk than paid-quarterly | Industry consensus; HFA segmented |
Paid-quarterly / contract-based | Month-3 dip masked until contract renewal | Industry consensus |
In-person (supervised) | Lower Month-3 risk than async online | Supervision moderates the signal |
Online/hybrid async | Highest Month-3 cliff | ABC Trainerize 2026 |
The bottom two rows matter most for the average online coach: async online and hybrid clients show the highest documented Month-3 cliff. That is the operational ground truth of an async coaching business in 2026.
The Dollar Cost of Month-3 Churn
The retention literature is fluent in percentage points but poor at translating them into dollar figures. The Bain-origin framing ("a 5% increase in customer retention can boost profitability by 25-95%" [Reichheld / Bain & Company, 1990-2024]) is correct but underspecified for personal training. Run the math on a realistic roster and the lever becomes visible.
A trainer charging $250/month, carrying 30 clients, on a target 12-month average tenure, represents $90,000/year in recurring revenue. Assume 4 of those 30 churn at Day 75 instead of Day 365. Direct revenue loss: 9 × $250 × 4 = $9,000 in already-acquired revenue. The smallest of three losses.
Add acquisition cost to replace those four. The "5x acquisition vs retention" figure (CloudGymManager, WellnessLiving, Mevolife 2025-2026) translates in personal training to roughly $200-400 per replacement client. Four: $800-1,600. Add the referral pipeline that does not get built. Communipass 2026 estimates each client retained past Month 6 produces 0.5-1 referral over tenure [Communipass, 2026]. Four lost retained clients = 2-4 lost referrals. At $2,250 referral LTV (9 × $250): $4,500-9,000 foregone revenue.
Total dollar cost of 4 Month-3 churns: $14,300-19,600. On a $90,000/year roster, that is 16-22% of total annual revenue, structurally gone from the predictable Day 60-90 inflection every roster encounters every cycle.
The 30-day vs 90-day vs 180-day comparison clarifies why Month 3 is the worst point on the LTV curve. A 30-day churn yields 1 month ($250), costs ~$300 acquisition, zero referrals: small, usually onboarding fit, recoverable. A 90-day churn (this article's window) yields 3 months ($750), costs the same acquisition, sits in the dead zone: too late to recover by communication, too short for a referral. A 180-day churn yields 6 months ($1,500), amortizes acquisition further, produces ~0.3-0.5 referrals. The 90-day churn is structurally the worst point on the LTV curve, and the most preventable.
Run the lever the other direction. A single Week-8 pivot that retains 2 of those 4 at-risk clients moves the math from $14,300-19,600 lost to $7,150-9,800 lost: a 50% reduction. Over a year: $7,000-10,000 in protected revenue per cycle. Over a 5-year horizon, that compounds into the largest retention lever most coaching practices have access to.
The 30-Client Wall Operations Playbook leaves this un-modeled: it covers HOW to scale to 30+ clients, but the retention curve is the demand-side input that determines whether those clients exist by Month 6. The intensity-prescription tool in RPE vs RIR for Online Coaching pairs with this macro-cycle decision. The pricing-vs-positioning analysis covers the front-end side of LTV (close rates, deal size); the Month-3 wall is the back-end side. Pricing fixes do not move the retention curve. The Week-8 pivot does. The Month-3 Churn Audit operationalizes this math at the roster level: inputs are monthly fee and current 30/60/90-day retention; outputs are the dollar cost of your Month-3 churn rate plus the projected ROI of pivot implementation.
Why "Motivation" Is the Wrong Diagnosis
Read any retention guide from the last five years and you will find the same advice: better check-ins, more accountability, stronger community, gamification streaks, win-back campaigns, monthly progress photos. The advice is not wrong. It is incomplete, and at Month 3, incompleteness is fatal.
The conventional retention playbook treats Month-3 churn as a behavioral problem. The data says it is a physiological problem expressed as a behavioral symptom. Behavioral interventions on physiological problems consistently underperform. That is what the BJ Fogg and Wendy Wood behavior-change literature actually says, read past the first chapter.
The Conventional Retention Playbook (And Why It Fails Here)
Gamification and streak mechanics work before the dose-response decay hits. They stop working when the underlying behavior is no longer producing the validating outcome the streak is supposed to reinforce. A client who hits a 60-day streak and then hits Week 9 with no body-comp change does not respond to a 70-day streak prompt; they respond to the absence of the result.
Increased check-in cadence is a communication tool. Communication does not change the body's response to a fixed stimulus. A daily check-in cannot make a Week-8 program produce Week-1 gains.
Accountability calls and weekly Zooms are time-intensive, do not scale past 20-25 clients, and address the symptom (commitment) not the cause (dose-response decay). Sam's $250/month client cannot economically receive a weekly 30-minute Zoom across a 30-client roster.
Win-back campaigns are reactive by definition. The client has already left the curve. Recovery rate from win-back campaigns in fitness coaching is documented at 5-12%, a structural ceiling no email copy improves. The right time to intervene is Week 7 (Day 49), not Week 14 (Day 95).
What the Behavior-Change Literature Actually Says
BJ Fogg's Behavior Model (Stanford Behavior Design Lab, the canonical framework used by every major behavior-change product since 2009) is Behavior = Motivation × Ability × Prompt [Fogg, 2019; behaviormodel.org]. When ability is mismatched to demand, motivation drops in response to the mismatch, not as the cause. The framework explicitly predicts what the retention data observes: a fixed-stimulus program in Month 3 produces an ability/demand mismatch as the stimulus drifts below the threshold that produces adaptation, and motivation follows downward.
Wendy Wood's habit research at USC (Good Habits, Bad Habits, 2019) and the foundational Lally et al. (2010) study in the European Journal of Social Psychology are similarly clear. Median time to habit automaticity is 66 days, range 18-254 days [Lally et al., 2010, PMC3505409]. Day 75 is the moment the new routine encounters its first true behavioral test. If the program is still producing strong adaptation feedback at Day 75, the routine survives. If the program has accommodated, the test arrives precisely when the validating biology has stopped supporting it. ACE Fitness 2025 reinforces this: complex health behaviors take substantially longer than 66 days to become automatic, often 12+ weeks. The 66-day mark is when the behavioral specificity test starts [ACE Fitness, March 2025]. The behavioral integration window sits on top of the dose-response decay window.
The Synthesis: Motivation Decay as Symptom, Not Cause
The conventional advice asks: "How do I keep my client motivated past Month 3?" The correct question is: "How do I keep the dose-response curve productive past Week 8, so the validating biology continues to support the routine while it integrates?"
The motivation playbook is not wrong. It is solving a downstream symptom of an upstream physiological event. When the dose-response curve is healthy, motivation interventions amplify the effect. When the dose-response curve has decayed, motivation interventions cannot produce the biology to support the behavior. The order matters. Programming first. Behavior second.
The same structural insight appears in the systems-vs-program thesis from a different angle: sometimes the system is not the problem; sometimes the physiology is, and Month 3 is where you find out. The progression-side diagnostic in Why Your Clients Are Not Progressing covers one of the four root causes named below; the 80/20 of Training Results names adherence as the highest-leverage outcome variable. The Month-3 wall is where adherence collapses if programming has not pivoted.
The Four Physiological Transitions of Week 8-12
Four things happen between Week 8 and Week 12 that did not happen between Week 1 and Week 7. They happen in every client who completes a fixed-stimulus mesocycle, at different intensities depending on training age, recovery capacity, and life context. The coach's job is to name which one is dominant and pivot accordingly. Month-3 churn is four events stacked on top of each other in the same window.
Transition (a): Original-Stimulus Accommodation (MEV Drift Upward)
The minimum effective volume (MEV) for hypertrophy adaptation drifts upward across a mesocycle. The 10-12 weekly sets that produced strong adaptation in Week 1 are sub-threshold by Week 8-10 for an intermediate trainee. The stimulus is no longer producing the adaptation it was producing originally.
Schoenfeld, Ogborn, and Krieger (2017, Journal of Sports Sciences) established the dose-response relationship between weekly resistance training volume and hypertrophy [PubMed 27433992]. Israetel and colleagues at Renaissance Periodization formalized the MEV/MAV/MRV framework; Greg Nuckols' Stronger by Science 2024-2026 syntheses translate it into the accumulation-deload-pivot cycle. Pelland et al. 2024 (Sports Medicine) confirmed periodization-with-variation outperforms linear progression at the 8-12 week mark [PubMed 41343037]. The ACSM 2026 Position Stand on Resistance Training (first update since 2009, built from 137 systematic reviews) explicitly endorses phase periodization [ACSM, 2026, PMC12965823].
Time horizon: 6-10 weeks for intermediate hypertrophy. 4-6 weeks for advanced. 8-14 weeks for novice (who have a different recovery curve, see transition b). On a check-in: "Felt easy this week" repeated without a corresponding load progression. Velocity on logged sets stable or improving without hard sessions. Body-comp and strength metrics flatten despite consistent attendance.
Transition (b): Recovery Cost Accumulation
Cumulative fatigue accumulates across the accumulation phase. The recovery dose appropriate for Week 1 is insufficient for Week 8, where fatigue has compounded across 7-8 mesocycles of sets. Sessions feel disproportionately hard relative to the load on the bar. RPE drifts upward at constant load.
Evidence base: Helms phase progression model (foundational 2015, updated 2020-2024); ACSM 2026 Position Stand on phase periodization; the systemic recovery literature in Recovery as a Growth Lever. NEAT compensation is one downstream-symptom path: when recovery cost accumulates, NEAT compensates downward, the deficit closes, and body-comp progress stalls without the coach seeing the upstream cause. The 7-variable Off-Program Leverage Hierarchy maps directly to which clients accumulate recovery cost faster.
Time horizon: highly variable, faster in clients with poor recovery infrastructure. On a check-in: "Felt heavy" repeated at constant load. Client reports needing extra rest days. RPE drifts up by 0.5-1.0 points without a programming change. Sleep complaints emerge.
Transition (c): Behavioral Specificity Test (66-Day Habit Horizon)
At Day 66, give or take, the new routine encounters its first true behavioral test. The novelty motivation has decayed. The social-approval boost has decayed. The routine now competes with the rest of life on equal terms. If the program is still producing validating biological feedback, the routine survives. If (a) and (b) have already hit, the test arrives at the worst possible moment.
Wood (2019), Good Habits, Bad Habits; Lally et al. (2010), median 66 days to automaticity, range 18-254 days [PMC3505409]; ACE Fitness March 2025 habit-formation guide; Fogg Behavior Model on motivation-decay timing.
Time horizon: Day 60-90 cluster, high variance with routine complexity. On a check-in: compliance gaps. Sessions skipped without explicit reason. "Got busy" messages. The standard goodbye prefix. App engagement drops 30-50% before logging stops entirely.
Transition (d): Adherence-Fatigue Interference (Data Layer Corruption)
Logging compliance degrades as the client experiences (a), (b), and (c). The coach's diagnostic data (RPE, RIR, session-level effort, body-comp updates) corrupts because the client logs inconsistently or with reduced fidelity. The coach cannot see (a), (b), or (c) because adherence-fatigue interference is hiding them in the data layer. This is the meta-transition: it corrupts the coach's ability to detect the other three.
Evidence base: practitioner consensus from coaching platforms; ABC Trainerize 2026 data on adherence-feature usage decay; the logging-friction literature in RPE vs RIR for Online Coaching. The repeated-bout-effect literature [Refoyo Roman et al., 2024, Sports Medicine, PubMed 38876249] predicts the diminishing-returns side: when stimulus is no longer novel, perceived session value degrades, reinforcing the logging dropoff.
Time horizon: begins Week 5-7, accelerates Week 8-12. On a check-in: logging gaps. Empty notes. Sessions logged with "felt good" and nothing else. Body-comp photos stop. The check-in becomes a one-way message rather than a two-way diagnostic exchange.
The Synthesis the Coach Has to Internalize
Clients quit at Month 3 for one structural reason masquerading as four behavioral ones: the program that started on Day 1 is no longer the correct dose for the body the client has on Day 75. The four physiological transitions of Week 8-12 are:
Original-stimulus accommodation (MEV drift upward; Week 1 stimulus is now sub-threshold)
Recovery cost accumulation (cumulative fatigue exceeds original recovery dose)
Behavioral specificity test (66-day habit horizon; program competes with rest of life on equal terms)
Adherence-fatigue interference (logging compliance degrades, corrupting the data the coach uses to detect 1-3)
Each transition requires a specific programming pivot at Week 8. Motivation interventions solve none of them. Most coaches see (d) first because it is the most visible: logging stops. They interpret it as motivation failure and intervene at the behavioral layer, missing the upstream (a), (b), and (c) that produced (d) in the first place. The correct sequence: diagnose which of (a), (b), (c) is dominant, pivot programming on that axis at Week 8, and (d) resolves as a side effect. This is the same diagnostic discipline in What Elite Coaches Do Differently: the meta-cognitive triage that separates senior decision-making from reactive intervention.
The 4-Layer Diagnostic Framework
Halfway through. Download The Month-3 Churn Audit. It converts this 4-question protocol into a roster-level scoring tool. Score your entire client book in 20 minutes; output is each client's pivot-recommendation by name.
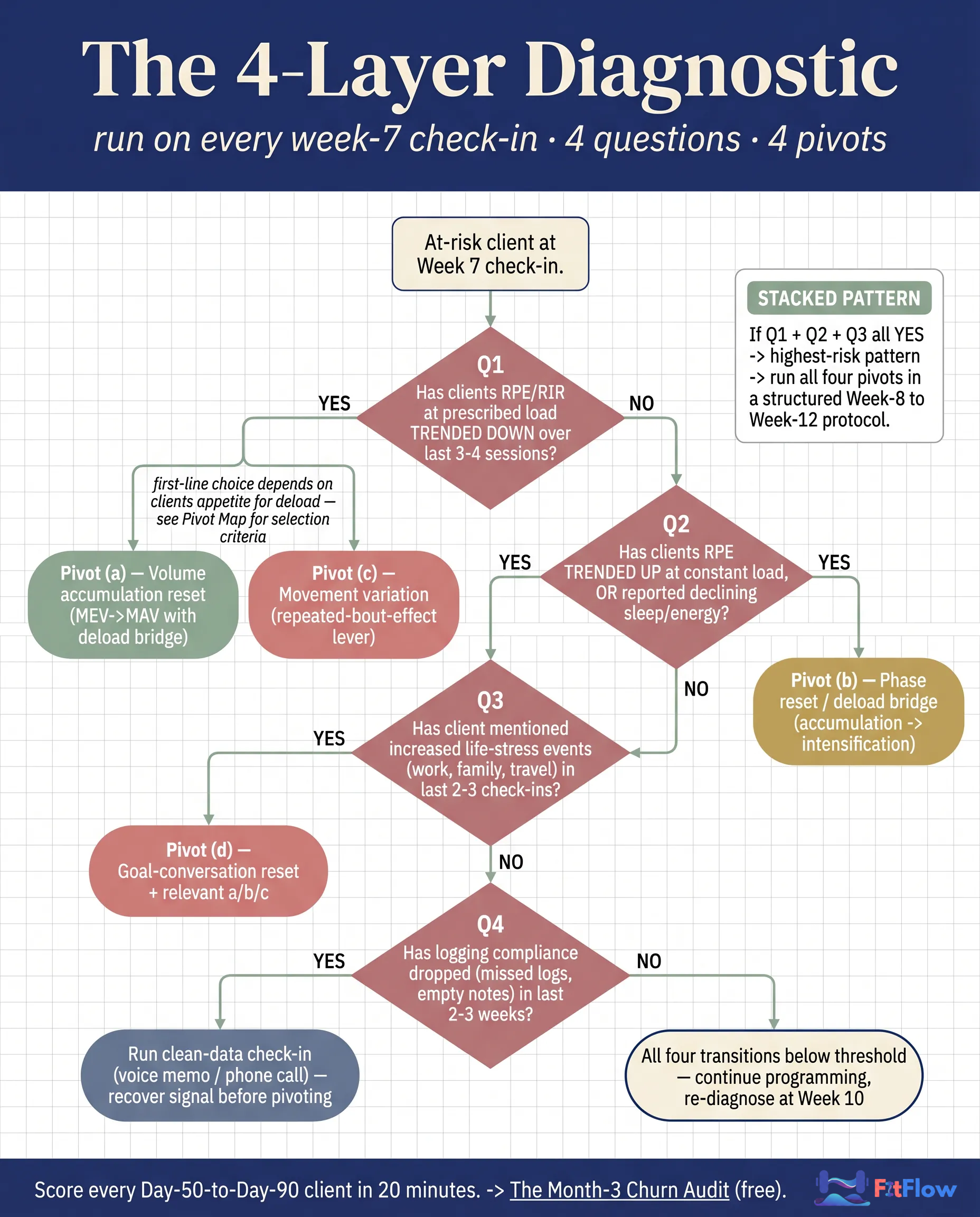
The framework does not replace your judgment. It structures it. Ask these four questions for each at-risk client at the Week-7 check-in. Run all four; the dominant route is determined by the priority rules in the decision table below (Q3 overrides; stacked YES patterns trigger combined pivots).
The Four Diagnostic Questions
Q1 (diagnoses transition (a), original-stimulus accommodation): Has the client's reported RPE/RIR at the prescribed load trended down across the last 3-4 sessions for the same exercise?
YES → original stimulus has accommodated. Route to Pivot (a) Volume accumulation reset, OR Pivot (c) Movement variation.
NO → continue to Q2.
Q2 (diagnoses transition (b), recovery cost accumulation): Has the client's reported RPE/RIR at the prescribed load trended up across the last 3-4 sessions, or has the client reported declining sleep, energy, or perceived recovery?
YES → cumulative fatigue is overtaking the original recovery dose. Route to Pivot (b) Phase reset.
NO → continue to Q3.
Q3 (diagnoses transition (c), behavioral specificity test): Has the client mentioned increased life-stress events (work, family, travel, sleep disruption) in the last 2-3 check-ins, independent of training performance?
YES → behavioral integration test arriving early or hot. Route to Pivot (d) Goal-conversation reset PLUS one of (a)/(b)/(c).
NO → continue to Q4.
Q4 (diagnoses transition (d), data layer corruption): Has the client's logging compliance dropped (missed logs, empty notes, late check-ins) in the last 2-3 weeks?
YES → data layer is corrupted; treat (d) as a signal of (a)/(b)/(c), not the primary diagnosis. Run a clean-data check-in (voice memo, phone call, simplified single-question check-in) to recover signal before pivoting.
NO → all four transitions are below threshold; continue current programming through Week 10 and re-diagnose.
The Decision Output Pattern
Pattern | Dominant Transition(s) | Programming Pivot |
|---|---|---|
Q1 YES, Q2 NO | (a) accommodation only | Pivot (a) Volume reset OR Pivot (c) Movement variation |
Q2 YES (regardless of Q1) | (b) recovery cost | Pivot (b) Phase reset / deload bridge |
Q3 YES (regardless of others) | (c) behavioral test hot | Pivot (d) Goal-conversation reset + relevant a/b/c |
Q4 YES alone | (d) data layer corrupted | Clean-data check-in first; do not pivot yet |
Q1 + Q2 + Q3 YES | Stacked transitions | Run all four pivots in a Week-8-to-Week-12 protocol |
The protocol takes 4-6 minutes per client once embedded in your Week-7 check-in form. Across a 30-client roster (8-12 clients in the Day 50-90 window at any given time), that is 30-60 minutes of structured diagnostic work per week, versus the 4-5 hours per client per quarter coaches typically spend on behavioral retention. The labor math pays for itself in the first cycle.
The intensity-prescription companion is RPE vs RIR for Online Coaching, the per-session calibration tool that determines whether the RPE/RIR data feeding Q1 and Q2 is reliable. The per-session tool produces the data; this macro-cycle tool consumes it.
The Week-8 Programming Pivot Map
The diagnostic tells you WHICH transition is dominant. The pivot map tells you WHAT to change, HOW to communicate it, WHEN it lands across the next four weeks, and WHAT to measure to verify the pivot worked.
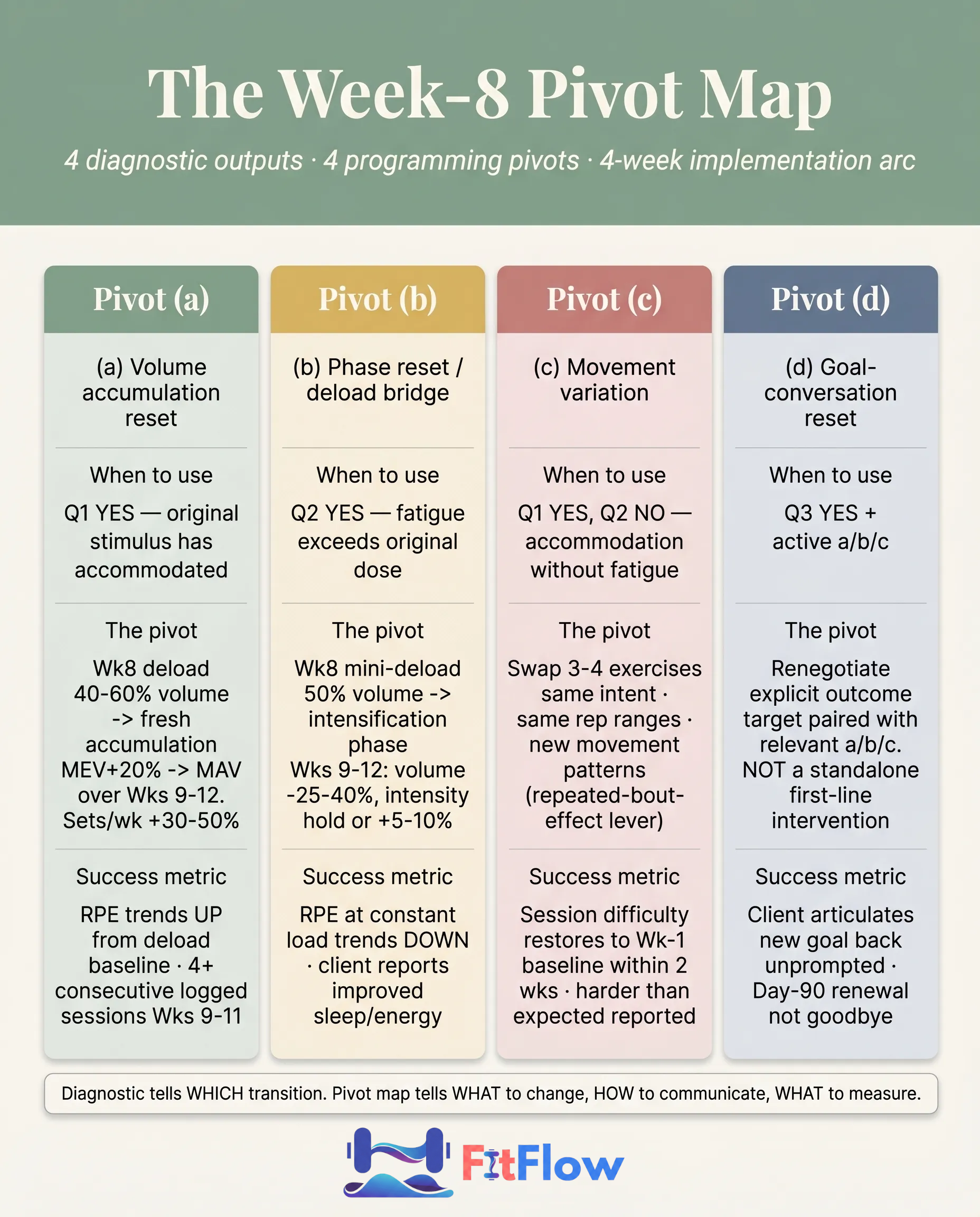
Pivot (a): Volume Accumulation Reset (MEV → MAV with Deload Bridge)
When to use. Q1 YES. Original stimulus has accommodated.
The pivot. One-week deload (40-60% of typical volume, same exercises), then a fresh accumulation block starting at the client's CURRENT MEV (revised upward) and progressing to MAV over 4-6 weeks. Sets per muscle per week typically increase 30-50% from the original block. Example: a client training 12 sets/week per major muscle resets to 6 in the deload week, then accumulates to 14-16 over Weeks 9-12.
Client communication. "Your body has adapted to the current volume. We are taking a deload week to clear fatigue, then restarting with slightly higher weekly volume to keep the gains coming. This is on purpose, not a setback. It is the difference between a program that keeps producing and a program that flattens."
Next 4 weeks. Week 8: deload (40-60% volume). Week 9: MEV+20%. Week 10: MEV+35%. Week 11: MAV. Week 12: MAV with deload check.
Success metric. Session RPE trends up from the deload baseline; load progression resumes; client logs 4+ consecutive sessions in Weeks 9-11 without compliance gaps.
Pivot (b): Phase Reset (Accumulation → Intensification or Recomp/Maintenance)
When to use. Q2 YES. Cumulative fatigue is overtaking the original recovery dose.
The pivot. Transition from accumulation to intensification (lower volume, higher relative intensity), OR insert a 4-6 week recomp/maintenance phase before re-entering accumulation. Total weekly volume drops 25-40%; load and intensity hold or rise slightly. Example: a client doing 16 sets/week at moderate intensity transitions to 9-12 sets/week at RPE 8-9, top-set focus, with 1 backoff set rather than 3.
Client communication. "You have accumulated a lot of work over 8 weeks, and your body is telling us through the recovery signals. We are shifting gears for 4-6 weeks: less total volume, higher quality on each set, more recovery between sessions. The goal is to consolidate the gains you have built rather than push for more volume right now."
Next 4 weeks. Week 8: mini-deload (3-4 days, 50% volume). Weeks 9-12: intensification, 25-40% volume reduction, intensity hold or +5-10%.
Success metric. RPE at constant load trends down; energy and sleep improve; top-set load and AMRAP rep counts hold or improve.
Pivot (c): Movement Variation (Repeated-Bout-Effect Lever)
When to use. Q1 YES, Q2 NO. Stimulus has accommodated but recovery is fine. A good first-line pivot for strong-adherence clients who would resist a deload.
The pivot. Substitute exercises for the same training intent: same muscle groups, same rep ranges, same intensities, different movement patterns. Refoyo Roman et al., 2024, Sports Medicine (PubMed 38876249) confirms switching exercises restores the adaptive signal at the same prescribed volume. Example: back squat → safety-squat-bar squat or front squat. Bench press → low-incline DB press or floor press. RDL → single-leg RDL or good-morning.
Client communication. "Your body has gotten efficient at the current movement patterns, which is great; it means you have adapted. To keep building, we are swapping a few exercises for the next block. Same muscles, same effort, slightly different pattern. The next block will feel harder than the previous program even at similar loads."
Next 4 weeks. Week 8: swap in 3-4 new exercises. Weeks 9-12: standard accumulation arc on the new pattern.
Success metric. Session RPE restores to Week-1 baseline within 2 weeks; client reports the swap as "harder than expected"; logging compliance returns.
Pivot (d): Goal-Conversation Reset (ONLY After a/b/c)
When to use. Q3 YES AND one of (a)/(b)/(c) is also active. Not a standalone first-line intervention.
The pivot. Renegotiate the explicit outcome target. The intake goal may no longer match the client's life context at Day 75. Move from "lose 15 lbs by August" to "establish a sustainable 3x/week training pattern through your busy season, then re-set body composition goals at Week 14." This sits downstream of (a)/(b)/(c). Without fixing the underlying dose-response problem first, the goal renegotiation becomes "managing decline" rather than "preserving the curve."
Client communication. "We set your goal at intake, and your life since then has shifted (name specifics). Let us reset the target to match where you are now, not where you were on Day 1. The training program is going to pivot too (name a/b/c specifics). Combined, the next 4-6 weeks have a realistic target that keeps you on the curve."
Next 4 weeks. Week 8: goal-reset conversation (15-30 min) combined with the relevant a/b/c programming pivot. Weeks 9-12: ride the revised target with the revised programming.
Success metric. Client articulates the new goal back unprompted; logging compliance returns; the Day 90-120 renewal conversation produces a renewal rather than a goodbye.
The Two-Client Case Study: Same Coach, Same Roster, Different Layer
Same coach (Sam). Same 12-week macrocycle. Client A and Client B are near-identical at intake: 19 months training experience, 3x/week online coaching, $250/month, hypertrophy-focused. Both hit Day 72 with the same warning signal: missed Week-7 check-in, "felt heavy" notes on the last three logged sessions, one "let me get back on track next week" message. The intervention layer is the only difference.
Client A: Conventional Retention Playbook
Sam runs the conventional playbook. Week 8: a check-in nudge, a personal voice memo, a discounted catch-up week, a Zoom call to "re-engage," a streak-tracking gamification reminder. Sam does not touch the programming.
Week 10: Client A logs two sessions, then one, then none. Sam sends a second voice memo, a third, a fourth. Each one is well-crafted, each on time. None of them changes the underlying physiology. Day 88: Client A cancels. "I just haven't been able to keep up." Sam attributes the loss to motivation failure. Total time invested: 4-5 hours over Weeks 8-12. Outcome: $0 recovered. Replacement acquisition: $300. Lost referral pipeline: ~$2,250 expected LTV.
Client B: Week-8 Programming Pivot

Sam runs the 4-question diagnostic on Client B's Week-7 data.
Q1 (RPE/RIR trending down?) → YES. Last 3 sessions show RPE 6.5-7 at loads that pulled RPE 8 in Week 4.
Q2 (RPE/RIR trending up or recovery declining?) → NO. Sleep stable. Energy fine.
Q3 (Life-stress events?) → NO.
Q4 (Logging compliance drop?) → Mild. One missed check-in.
Diagnostic output: transition (a) dominant. Pivot: (a) plus (c) combined. Week 8: deload (40% volume). Weeks 9-12: fresh accumulation block with 3 exercise swaps (safety-bar squat replacing back squat; low-incline DB press replacing flat bench; single-leg RDL replacing standard RDL).
Sam sends one message at Week 8: "Your body has adapted to the current block. We are taking a deload week, then coming back with a fresh block that includes a few new exercises. This is on purpose. The next block will feel harder than the last even at similar loads."
Day 90: Client B logs three consecutive sessions. Notes: "These new exercises are kicking my ass." Compliance restored. Day 120: renewed for another quarter, reports strength gains on the new variations. Total time invested: ~45 minutes over Weeks 8-12. Outcome: $750 recovered, referral pipeline preserved.
The Comparison
Metric | Client A (Conventional) | Client B (Week-8 Pivot) |
|---|---|---|
Diagnostic at Week 7 | None | 4-question diagnostic |
Intervention layer | Behavioral | Physiological |
Programming change Week 8 | None | Deload + 3 exercise swaps |
Day-90 outcome | Cancelled | Compliance restored (3 consecutive logged sessions) |
Day-120 outcome | Lost (replacement cost incurred) | Renewed for another quarter; referring |
Coach time invested | 4-5 hours over Weeks 8-12 | ~45 minutes over Weeks 8-12 |
Quarter revenue outcome | -$750 + ~$300 replacement acquisition | +$750 + intact referral pipeline |
LTV impact | ~$2,250 lost + 0.5-1 referrals | LTV preserved; referrals intact |
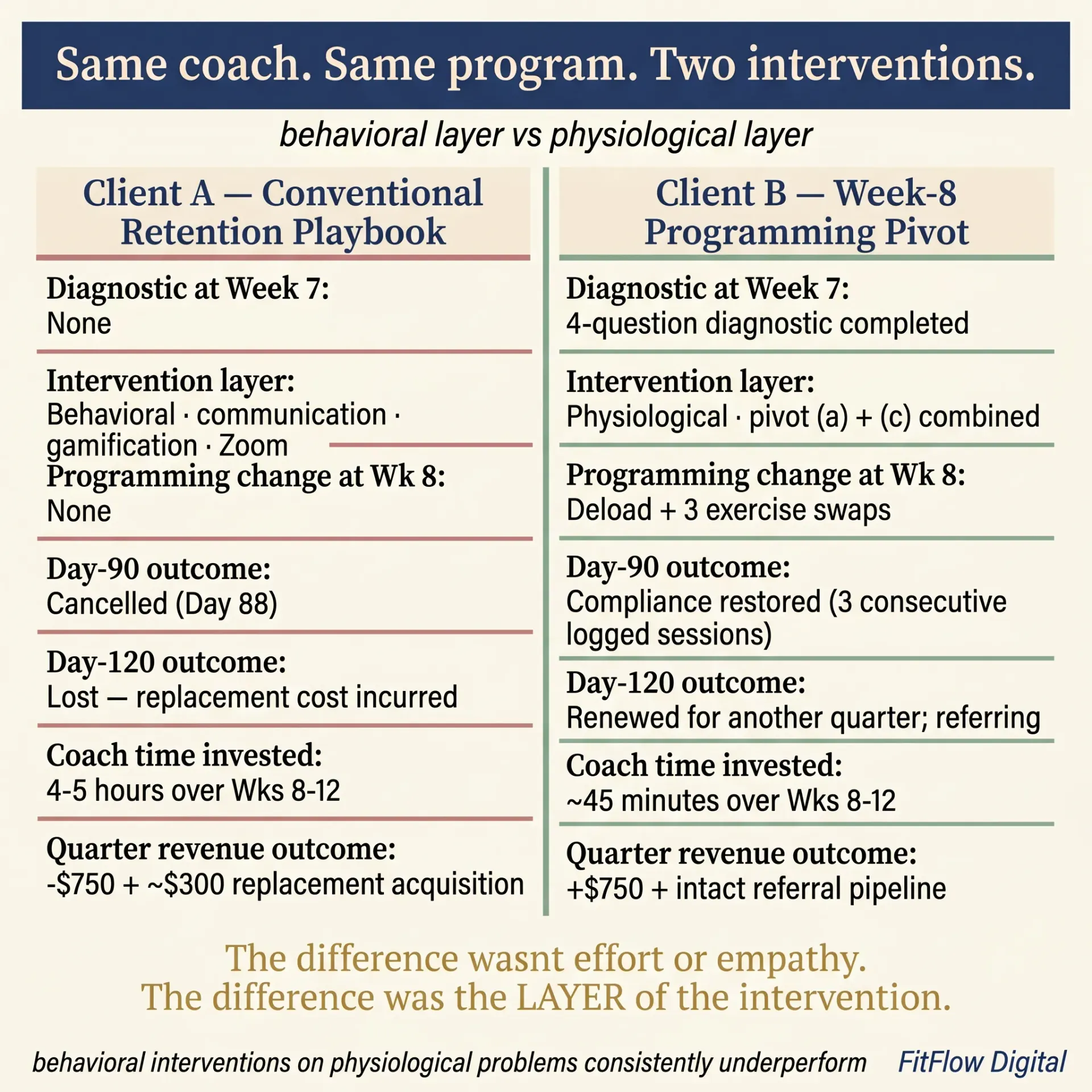
The difference was not the coach's effort or empathy. Sam actually invested more time in Client A's behavioral intervention than in Client B's physiological pivot. The difference was the layer. Behavioral interventions on physiological problems consistently underperform; programming pivots on dose-response problems consistently work. This is the same structural insight named in Why Most Hypertrophy Programs Fail After 6 Weeks: the Week-6 plateau and the Month-3 wall are parallel mechanisms at different thresholds. Both are predictable; both have programming fixes.
The Diagnostic in Practice: Week 8 to Week 12 Implementation
Most coaches read a piece like this and change nothing because they do not know where to start. Here is the week-by-week operational plan.
Week 0 (Now): Modify Your Existing Check-In Form
Add four fields to your standard Week-7 check-in (or your bi-weekly check-in, if that is your cadence): one for each diagnostic question (Q1-Q4). Use the exact wording from the diagnostic section. Each question is a yes/no with a one-line "why" prompt. The check-in form modification takes 10-15 minutes in any major coaching platform. Set a recurring reminder: every Week 7 of every client's onboarding cycle, run the 4-question diagnostic before the Week-8 programming decision.
Week 1: Build the Pivot Templates
Create a saved program for each of the four pivots in your coaching platform (most allow templates applied in 2-3 minutes per client).
Pivot (a): Week 8 deload + Weeks 9-12 fresh accumulation at MEV+20%-MAV.
Pivot (b): Week 8 mini-deload + Weeks 9-12 intensification with 25-40% volume reduction.
Pivot (c): same structure but with 3-4 exercise swaps.
Pivot (d): goal-reset conversation script + programming change overlay.
Week 2: Run the Audit on Existing At-Risk Clients
Pull your roster. Score every client in the Day 50-90 window on the 4 diagnostic questions using their most recent check-in data. Tag each at-risk client with the dominant transition and the recommended pivot. Day 75-90 clients: implement the pivot at the next session. Day 50-75 clients: schedule the diagnostic at Week-7 check-in and the pivot at Week 8.
Platform-Specific Integration Notes
Platform | Integration | Time Cost |
|---|---|---|
ABC Trainerize (Habit Tracking 2026 + adherence dashboard) | Add 4 custom check-in questions to the Week-7 template; create 4 saved programs for the pivots; map the adherence dashboard signal to the Q4 trigger | ~30 min setup |
Hevy Coach | Use client profile custom fields for the 4 diagnostic flags; create 4 program templates; rely on Hevy's RPE/RIR log for Q1/Q2 detection | ~20 min setup |
TrueCoach (2026 client dashboard refresh) | Intake form modification + saved workout templates; the 2026 dashboard refresh surfaces compliance signals that feed Q4 | ~25 min setup |
CoachRx (OPEX) (Q1 2026 programming-pivot templates) | Use the pre-built Q1 2026 pivot templates; add the 4 questions to the assessment workflow; simplified 1-5 RPE scale aligns with novice diagnostic | ~15 min setup |
Trainerize (legacy) | Use post-session RPE + custom check-in fields; saved programs for the 4 pivots | ~30 min setup |
One critical clarification on platform dashboards. The adherence dashboard in your coaching platform observes the consistency curve. It does not change it. Visibility is not intervention. The dashboard tells you which clients to run the diagnostic on; the diagnostic plus the pivot is what produces the renewal. Coaches who confuse dashboard visibility with retention intervention end up with detailed records of decline.
Population Variants
The 4-Layer Diagnostic and the Pivot Map are population-general. Each major sub-segment of the typical online coaching roster has a variant. One framework, four populations, four variants. The dominant transition shifts by population.
GLP-1 Medication Clients (Doubled Month-3 Risk)
GLP-1 efficacy plateaus typically arrive between Months 2-4 during dose titration (often weeks 2-8 in early plateau form, full plateau Months 6-12 per NEJM longitudinal data, Wadden et al. STEP trials [NEJM, 2021-2024]). Transition (b) recovery cost accumulation AND the medication plateau hit in the same window: two distinct plateaus converging.
Run Pivot (b) phase reset, but extend the recomp/maintenance phase to 6-8 weeks instead of 4-6. The medication-driven energy and recovery profile makes the standard accumulation arc unsustainable. Pivot (d) goal-conversation reset is also essential: body-comp targets that ignored the medication plateau need to be reframed against the actual medication trajectory. For the full GLP-1 framework, see the GLP-1 personal training coaching guide.
Novice Clients (Under 12 Months Training Experience)
Novices accumulate recovery cost faster per absolute load than intermediates. Transition (b) typically arrives earlier than the canonical Week 8-10, often Week 6-8.
Run the diagnostic at Week 6 instead of Week 7. Use Pivot (a) or Pivot (c) more aggressively. Avoid Pivot (b) intensification: load demands are not yet appropriate for novices. Conti et al. 2026 (preprint) confirms training consistency in the first 28 days is the strongest predictor of long-term adherence; that is where to invest disproportionate attention for the novice segment.
Intermediate Hypertrophy Clients (12-24 Months Training)
The canonical population. All four transitions arrive close to their typical Week 8-12 timing. Standard application. Pivots (a) and (c) most often dominant. Pivot (b) for clients with poor recovery infrastructure. Pivot (d) only when Q3 is YES.
Recomp / General-Fitness Clients (Goal-Diffuse)
Without a sharp body-comp or strength target, transition (c), the 66-day behavioral integration test, is the dominant transition. The dose-response decay is real but less salient because the validating feedback was always softer. Run Pivot (d) goal-conversation reset as the first intervention, paired with Pivot (c) movement variation. These clients benefit most from rotating training intent (strength → hypertrophy → conditioning) rather than a strict accumulation-deload cycle. Pain-modifier clients sit in a related sub-segment; see Program Around Chronic Pain Without Losing Intensity.
Your Next Steps
You now have the diagnostic and the pivot map. Here is how to make it operational across your entire roster this week.
Download "The Month-3 Churn Audit." It converts the 4-Layer Diagnostic Framework into a roster-level scoring tool. Every at-risk client (Day 50-90) gets scored on the four diagnostic questions. Output: each client's dominant transition and the recommended Week-8 pivot, by name, on a single one-page view. Built for coaches managing 20-50+ clients. Compatible with every major coaching platform (Trainerize, Hevy, TrueCoach, CoachRx, Trainerize legacy). Includes a built-in LTV math calculator that turns your current 30/60/90-day retention into the dollar cost of your Month-3 churn rate, plus projected ROI of pivot implementation. Free. Get the free Audit →
Three follow-up reads from the cluster:
Sister physiology diagnostic at a different threshold: Why Most Hypertrophy Programs Fail After 6 Weeks. The Week-6 plateau (neural-to-muscular phase shift) and the Month-3 wall (dose-response decay) are parallel mechanisms at different thresholds.
BG bridge, operational scaling counterpart: Online Coaches' 30-Client Wall Operations Playbook. The retention curve is the demand-side input to the 30-client wall's supply-side problem.
Per-session intensity tool that pairs with the macro-cycle decision: RPE vs RIR for Online Coaching. Intensity prescription is the per-session calibration tool. The Week-8 pivot is the macro-cycle retention tool. Run them in tandem.
The framework is not the work. The audit is. Run it this week. Re-read this article in 30 days, after the Week-0-to-Week-12 implementation has rolled through your at-risk cohort. The next time the goodbye-prefix message lands in your inbox at 6:43 a.m. on a Tuesday, you will already know which transition produced it and which pivot you should have run two weeks earlier. The curve is predictable. The intervention is specific. The Week-8 decision is yours.
Frequently Asked Questions
Comments