The Personal Trainer's Guide to GLP-1 Coaching: Evidence-Based Programming and Muscle Preservation
About 1 in 8 US adults now take a GLP-1 medication for weight loss, diabetes, or a related condition (KFF, 2025). If you manage a roster of 20 or more clients, the odds that at least one is on semaglutide, tirzepatide, or a related GLP-1 receptor agonist are no longer hypothetical -- they are a scheduling reality. With oral GLP-1 pills reaching 170,000 prescriptions within three weeks of their January 2026 launch (AAMC), that number keeps climbing. GLP-1 personal training is not a niche specialization anymore. It is a core competency.
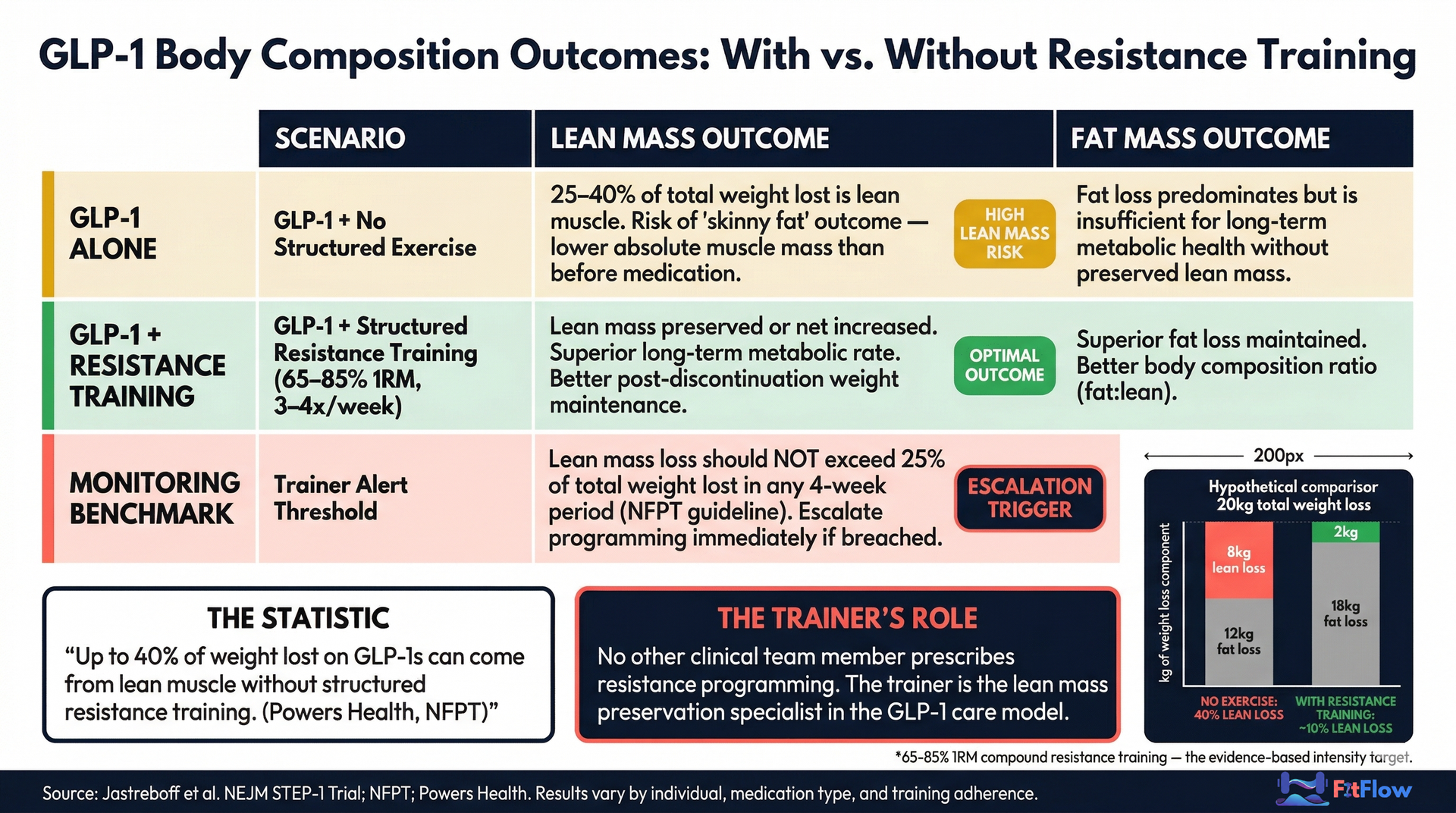
Here is the problem most trainers miss: up to 40% of the weight lost on GLP-1 medications can come from lean muscle mass when resistance training is absent (Powers Health; NFPT). The client's scale drops. Their body composition deteriorates. They end up lighter but weaker -- the "skinny fat" outcome that undermines metabolic health and long-term weight maintenance. Research shows 60% of lost weight is regained within 12 months of stopping GLP-1 therapy (eClinicalMedicine / Cambridge, 2026), and clients who lack a durable muscle foundation are the most vulnerable to that rebound.
This is your intervention point. No other member of the GLP-1 clinical team prescribes and delivers structured resistance programming. You are the lean mass preservation specialist.
This guide is the complete operational playbook: the clinical science you need to understand, the programming protocols you need to implement, the tracking framework that keeps clients on course, and the systems that make GLP-1 coaching scalable across your entire roster.
The GLP-1 Muscle Loss Problem — Why Trainers Are the Critical Intervention
The research is clear, and the scale of the problem demands attention.
The STEP-1 semaglutide trial (Jastreboff et al., NEJM) put specific numbers to the problem: lean mass fell roughly 9.7% while fat mass dropped about 19.3%. Fat loss leads, but the lean mass loss is clinically significant -- and it compounds without intervention. NASM reports that 30-60% of weight loss includes lean muscle when resistance training is absent. The range depends on starting body composition, protein intake, and activity level, but the direction is consistent across studies.
Sex-Specific Risk Profiles
Research from Johns Hopkins published in JAMA Internal Medicine found that women lose an average of 11% of their starting body weight on GLP-1s, compared to about 7% for men. Greater total weight loss means greater absolute lean mass risk, which creates different programming thresholds by sex. Women on GLP-1 medications may need earlier and more aggressive resistance training to protect lean mass.
The "Skinny Fat" Outcome
NASM's 2025 survey found that 50% of trainers working with GLP-1 clients report "skinny fat" outcomes -- clients who lost weight on the scale but lost disproportionate amounts of metabolically active muscle tissue. The clinical result: a lower resting metabolic rate, reduced functional strength, and a body composition that is actually worse from a health standpoint despite weighing less.
This is exactly why the discontinuation data matters. When clients stop GLP-1 therapy, 60% of lost weight is regained within 12 months (eClinicalMedicine / Cambridge). Clients who kept their lean mass through structured resistance training have a stronger metabolic base to resist that regain. Clients who lost muscle along with fat have less protection and are more likely to regain at a higher body fat percentage than before they started.
Scenario | Lean Mass Outcome | Fat Mass Outcome | Programming Implication |
|---|---|---|---|
GLP-1 alone (no exercise) | 25-40% of total weight lost is lean mass | Fat loss predominates but body composition deteriorates | Immediate resistance training intervention required |
GLP-1 + structured resistance training | Lean mass preserved or increased | Superior fat loss ratio maintained | Monitor body composition monthly |
Monitoring benchmark | Lean mass loss should not exceed 25% of total weight loss | At least 75-80% of weight loss should be fat mass | Adjust programming immediately if threshold is breached |
The Trainer's Role in the Care Model
The prescribing physician manages the medication. The registered dietitian manages the nutritional plan. The trainer manages the resistance programming that determines whether the client preserves lean mass or loses it. No other team member fills this role. In the multidisciplinary GLP-1 care model, the personal trainer is the muscle preservation specialist -- and the evidence supports the position that this intervention is clinically necessary, not optional.
The GLP-1 Client Intake Protocol — Setting Up Every Engagement Correctly
Get the Free GLP-1 Client Intake & Autoregulation Template: Download Free Template Kit
Standard intake forms miss critical data points for GLP-1 clients. A PAR-Q and basic fitness history will not capture the medication-specific variables that shape your programming decisions. Here is the intake framework built for this population.
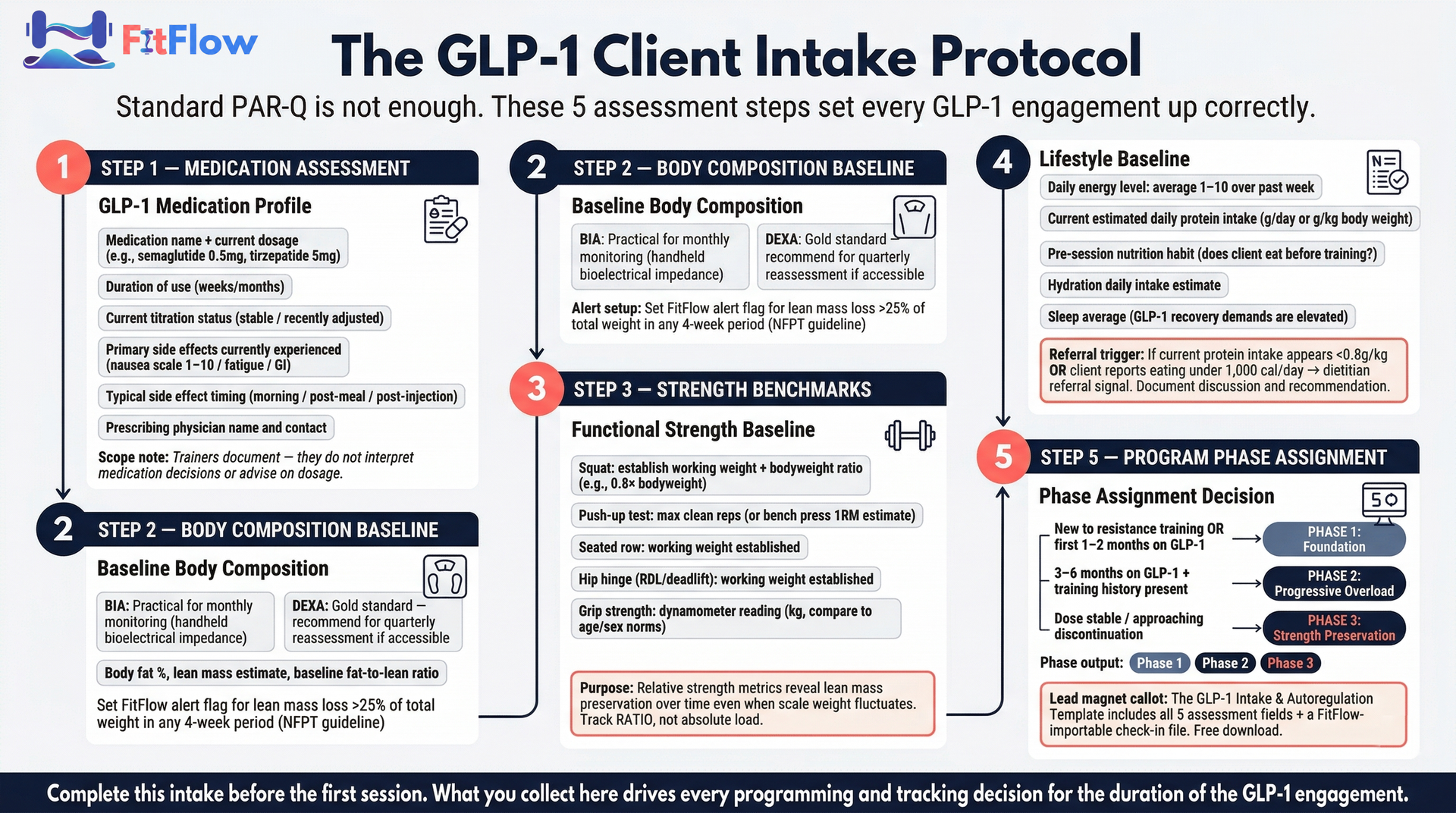
GLP-1-Specific Assessment Fields
Your intake for GLP-1 clients should capture the following beyond your standard form:
Medication details: Current GLP-1 medication name, dosage, duration of use, and upcoming titration schedule (dosage increases typically happen monthly and directly affect energy, nausea, and GI symptoms)
Side effect profile: Primary side effects currently experienced (nausea, fatigue, GI discomfort), typical timing relative to injection or pill day, and severity on a 1-10 scale
Protein intake estimate: Current daily protein intake in grams -- most GLP-1 clients severely under-eat protein due to appetite suppression, and this is your most actionable nutritional data point
Training status: Previous resistance training experience, current training frequency, and any periods of inactivity during GLP-1 initiation
Physician clearance: Confirmation that the prescribing provider has cleared the client for resistance training, with any specific activity restrictions documented
Body composition history: Weight trajectory since starting GLP-1 medication, not just current weight -- rate of loss matters for programming decisions
Baseline Assessment Protocol
Before writing a single workout, establish these baselines:
Body composition measurement: BIA scan (practical for monthly monitoring) or DEXA scan (gold standard; recommend quarterly). Record body fat percentage, lean mass in pounds or kg, and calculate the fat-to-lean mass ratio as your primary tracking metric.
Functional strength benchmarks: Squat-to-bodyweight ratio, push-up test (to failure or modified), grip strength (dynamometer), and a hip hinge movement assessment. These become your longitudinal lean mass indicators.
Energy level baseline: Client self-reports average daily energy on a 1-10 scale over the past week. This calibrates your intensity expectations and sets the reference point for RPE-based autoregulation.
Scope of Practice Note
This intake assesses movement capacity and training readiness. It does not assess medical status. Trainers do not interpret lab work, advise on medication dosage, or provide dietary prescriptions. If a client discloses information outside your scope -- cardiac symptoms, disordered eating patterns, psychological distress related to weight -- document the conversation and refer to the appropriate provider. Clear scope language protects both your client and your professional standing.
Evidence-Based Resistance Training Programming for GLP-1 Clients
This section is the operational core of the guide. The programming parameters below are drawn from NFPT, ACSM, and NASM sources, adapted for the specific physiological context of GLP-1 therapy.
Programming Parameters
Parameter | Specification | Rationale |
|---|---|---|
Intensity | 65-85% 1RM for compound movements | Sufficient to stimulate muscle protein synthesis without exceeding recovery capacity |
Volume | 2-4 sets per exercise, 6-12 reps (hypertrophy), 3-6 reps (strength) | Progressive volume drives adaptation; start conservative and build |
Frequency | 3-4 resistance sessions per week (minimum 2) | Below 2 sessions per week, lean mass preservation becomes difficult to sustain |
Recovery | 48-72 hours per muscle group | GLP-1 therapy increases physiological recovery demands; respect this |
Session duration | 30-45 minutes (early months); 40-50 minutes (adapted clients) | Shorter sessions are better tolerated during titration periods |
Exercise priority | Compound movements first: squats, deadlifts, rows, presses, hip hinges | Maximum anabolic stimulus per unit of training time |
The RPE-Based Autoregulation Protocol
GLP-1 clients have highly variable energy levels. Nausea, fatigue, and GI side effects shift with dosage titration cycles -- often on a weekly or biweekly rhythm. A fixed-intensity program will fail these clients on their worst days and underload them on their best.
RPE (Rate of Perceived Exertion) on a 0-10 scale is the go-to intensity management tool:
Typical working RPE target: 7-8 out of 10 (2-3 reps in reserve)
Adjustment trigger: If RPE for a normal working weight hits 9+ when it usually sits at 7-8, cut load by 15-20% for that session
Volume reduction protocol: On high-symptom days (nausea score 7+/10, energy score below 4/10), reduce total working sets by 20-30% and shift focus to movement quality over load progression
Non-negotiable rule: A reduced-intensity session is always better than a skipped session for lean mass preservation. The stimulus-to-fatigue ratio matters more than absolute load on any single day.
In practice: Your client walks in for her Tuesday session. Her pre-session check-in shows nausea at 6/10 and energy at 4/10 -- it is a titration week. Her typical squat working weight is 135 lbs at RPE 7. Today, 135 lbs feels like RPE 9. You drop to 115 lbs (about a 15% cut), keep the movement pattern, trim from 4 sets to 3, and log the adjustment. She still gets a muscle-preserving stimulus. She leaves feeling accomplished instead of beaten down. Next week, when energy rebounds to 7/10, you return to the standard protocol. That is autoregulation in action.
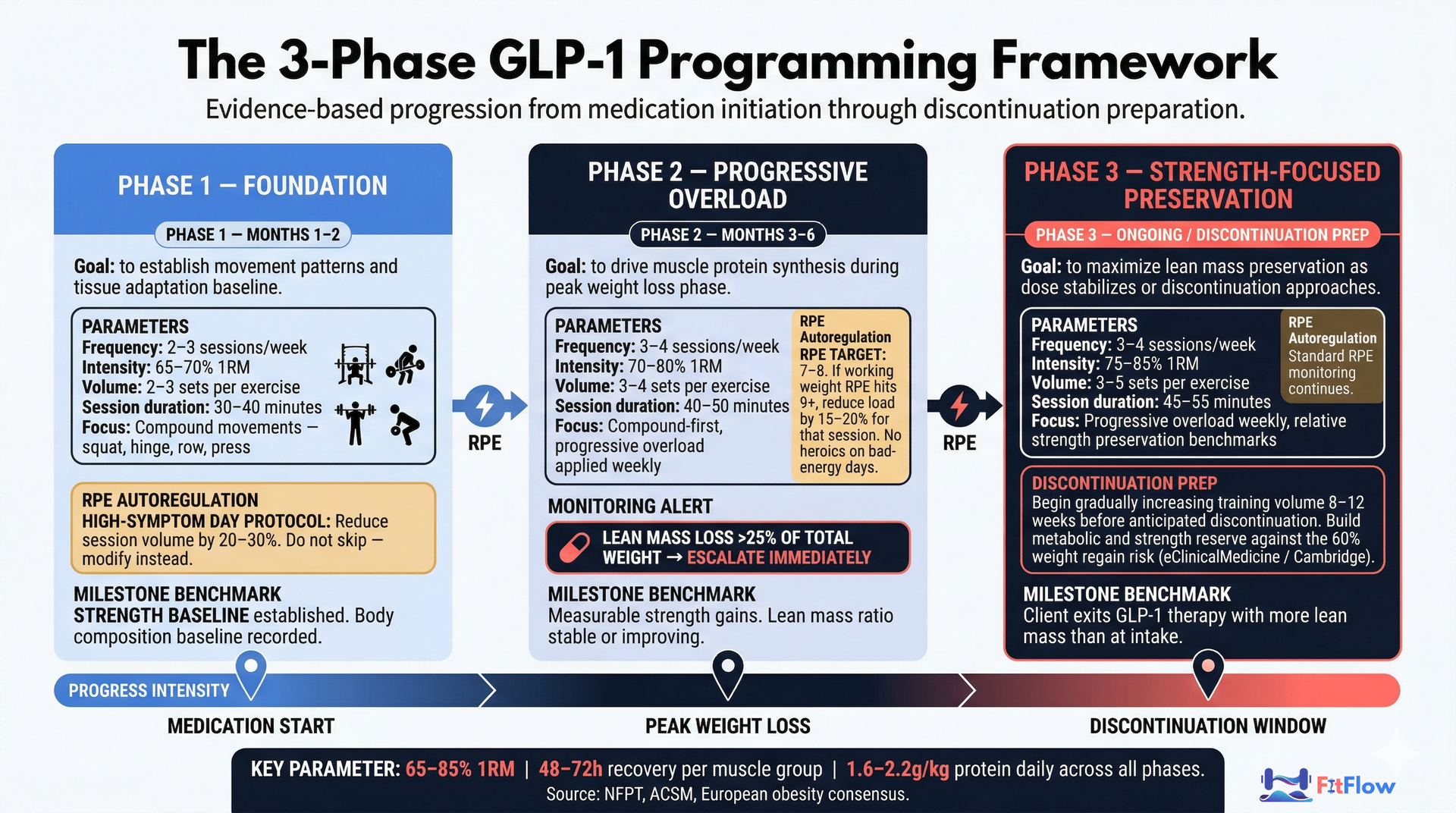
The Three Programming Phases
Phase 1 -- Foundation (Months 1-2 of GLP-1 use, or clients new to resistance training)
Goal: Establish movement patterns, build baseline strength, allow tissue adaptation
Protocol: 2-3 sessions per week, 2-3 sets per exercise, 65-70% 1RM, 30-40 minute sessions
Autoregulation: Cut session volume by 20-30% on high-symptom days; prioritize movement quality
Key focus: Compound movement proficiency, RPE tracking habit, protein intake awareness
Phase 2 -- Progressive Overload (Months 3-6)
Goal: Drive muscle protein synthesis, build measurable strength gains, protect lean mass during peak weight loss
Protocol: 3-4 sessions per week, 3-4 sets per exercise, 70-80% 1RM, compound-focused, 40-50 minute sessions
Autoregulation: RPE-controlled with weekly body composition trend review and relative strength checks
Key focus: Progressive overload tracking, monthly BIA monitoring, protein compliance audit
Phase 3 -- Strength-Focused Preservation (Ongoing / Discontinuation Preparation)
Goal: Maximize lean mass preservation as medication dose stabilizes or discontinuation approaches
Protocol: 3-4 sessions per week, 3-5 sets per exercise, 75-85% 1RM, weekly progressive overload
Discontinuation prep: Start increasing training volume and frequency 8-12 weeks before anticipated GLP-1 discontinuation to build metabolic and strength reserves against weight regain
Key focus: Strength-to-bodyweight ratio, body composition ratio stability, building movement habits that outlast the medication
For deeper methodology on periodization frameworks and volume landmark guidance, see our guide on evidence-based periodization principles and volume landmarks.
Nutrition Coordination — Protein, Timing, and Staying in Your Lane
GLP-1 appetite suppression creates a nutritional paradox: the medication that drives weight loss also mutes the appetite signals that would normally remind clients to eat enough protein. Many GLP-1 clients under-eat protein exactly when their body needs it most to support lean mass under resistance training.
Evidence-Based Protein Targets
Research from the European obesity research consensus and NASM guidelines recommends:
Minimum: 1.6 g of protein per kg of body weight per day
Optimal for lean mass preservation: 2.0-2.2 g per kg of body weight per day
Distribution: Spread across 3-4 meals -- front-loading protein at the meal before training is particularly important for muscle protein synthesis
For a 75 kg client, this means 120-165 g of protein daily. Most GLP-1 clients, when first assessed, consume 40-60 g per day -- a gap that undermines even well-designed resistance programming.
The Trainer's Role in Protein Guidance
Trainers can and should emphasize protein targets as part of fitness coaching. Frame protein intake as a "training foundation" -- the fuel that makes resistance work productive. This is well within scope.
Trainers should not build comprehensive meal plans unless they also hold a registered dietitian credential (RD/RDN). The line is clear: recommending a protein target is coaching; prescribing a caloric plan is dietetics.
The Referral Trigger
If a client consistently eats fewer than 1,000 calories per day due to GLP-1-driven appetite suppression, treat this as a dietitian referral signal. Document the discussion and your recommendation. Other triggers include suspected disordered eating, persistent fatigue that does not respond to programming changes, and any client expressing significant anxiety or distress around food or weight.
Practical Nutrition Notes
Pre-training: A protein-containing meal 2 hours before sessions. Avoid fasted training, especially during nausea-prone titration windows.
Hydration: GLP-1 clients often experience dehydration. Aim for 2.5-3L daily, plus 500-750ml on training days.
Timing around injection: Some clients hit peak nausea 24-48 hours post-injection. Schedule higher-intensity sessions for the days when GI symptoms are typically lowest.
The bottom line: your job is not to be the nutritionist. Your job is to make sure the resistance stimulus is matched by enough protein to make muscle protein synthesis possible. Without adequate protein, even optimal programming delivers suboptimal lean mass outcomes.
Body Composition Tracking — The Metrics That Actually Matter
Take the Complete GLP-1 Coaching Protocol With You: Download Free Template Kit
Scale weight is not enough for GLP-1 clients. A client who loses 15 lbs but 6 of those pounds are lean mass has a fundamentally different outcome than a client who loses 15 lbs with 14 from fat. The scale reads the same. The body composition -- and the long-term health trajectory -- are completely different.
The 6 Essential Tracking Metrics
Body composition (fat mass vs. lean mass): Monthly BIA scan or quarterly DEXA. Track the fat-to-lean mass ratio, not just total weight.
Relative strength metrics: Squat or leg press load relative to current body weight. Steady or rising absolute strength during weight loss signals lean mass preservation. Proportional drops signal lean mass decline.
Grip strength: Simple, objective, and strongly correlated with overall muscle mass. Use a hand dynamometer monthly. A declining trend is an early warning signal.
Protein compliance: Weekly self-reported protein intake in grams, tracked via check-in. This is the most actionable data point.
Energy and symptom log: Daily RPE and side-effect severity ratings. This drives autoregulation decisions and helps spot patterns relative to dosage timing.
Progress photos: Monthly, same conditions (lighting, time of day, clothing). Qualitative, but powerful for client motivation when the scale is misleading.
The Alert Threshold
If lean mass loss exceeds 25% of total weight lost in any 4-week monitoring period, treat this as an escalation trigger (NFPT guideline). The response:
Immediate protein intake audit
Review training adherence and session intensity data
Consider adding one resistance training session per week
If the trend continues a second month, recommend a DEXA scan and discuss findings with the client's medical team
Technology Integration
This tracking framework is where technology becomes operationally essential. Manually tracking six metrics across 10-20 GLP-1 clients is not sustainable. A purpose-built tracking dashboard changes the equation.
FitFlow's client dashboard supports body composition tracking fields built for GLP-1 clients -- body fat percentage, lean mass from BIA, relative strength benchmarks, and protein compliance scores. The weekly check-in system can include RPE, energy score, and protein intake questions, feeding data into the dashboard automatically. Alert thresholds flag clients whose trends show accelerated lean mass loss, prompting trainer review without manual data review for every client every week.
For the general tracking framework this GLP-1 protocol extends, see the 5-metric client progress tracking dashboard. For guidance on selecting BIA devices, DEXA scan services, and wearable integrations, see our guide on body composition tracking tools and your fitness tech stack.
ACSM ranked wearables as the #1 fitness trend in 2026. Trainers who integrate body composition monitoring and automated tracking into their GLP-1 coaching package are aligned with where the industry is heading -- and they are delivering a meaningfully higher standard of care.
Managing a GLP-1 Client Roster — The Operational Workflow
A single GLP-1 client requires more frequent monitoring than a standard training client. Multiply that across 5, 10, or 20 GLP-1 clients, and the operational load becomes the limiting factor -- not the programming knowledge.
Recommended Check-In Cadence
Weekly: Automated check-in (RPE, energy score, nausea severity, protein compliance, training adherence) via FitFlow or a similar platform
Monthly: Body composition reassessment (BIA scan) and relative strength benchmark review
Quarterly: DEXA scan (recommended), comprehensive programming phase review, and progress discussion
As needed: Real-time communication for symptom escalations (cardiac symptoms during exercise, severe persistent nausea, signs of disordered eating)
Session Adjustment Decision Rules
Establish clear rules in advance so you are not improvising during sessions:
Client-Reported Data | Programming Decision |
|---|---|
RPE 8+ for target working weight | Reduce load by 15-20% for that session |
Nausea score 7+/10 | Switch to technique-focused session at 50% intensity |
Energy score below 4/10 | Reduce total volume by 20-30%, maintain compound movements |
Missed 2+ sessions in a week | Consolidate into remaining sessions; do not try to "make up" volume |
Lean mass loss >25% of total weight loss (monthly review) | Escalate: protein audit + frequency increase + consider DEXA |
The Multidisciplinary Communication Framework
Professional GLP-1 coaching means knowing when to communicate and when to refer:
Know the prescriber: Document their name and contact information
Monthly clinical notes: When relevant changes occur (unusual muscle loss rate, severe fatigue limiting training), send a brief professional note to the prescriber. This is collaboration, not scope overreach.
Referral triggers:
Consistent energy below 3/10 across multiple weeks --> physician
Suspected eating disorder behaviors or consistently under 1,000 cal/day --> registered dietitian
Mood changes, anxiety around weight, body image distress --> behavioral health professional
Any cardiac symptoms during exercise --> physician immediately
The Time Math at Scale
A well-structured GLP-1 workflow using automated check-ins and dashboard alerts allows a trainer managing 20 GLP-1 clients to review all check-in data in under 45 minutes per week. Without this system, the same workload takes 3-4x the manual effort -- roughly 3 hours of individual follow-up, manual data review, and ad-hoc programming adjustments.
The Trainerize 2026 Industry Report found 64% of trainers already use or explore AI for backend tasks. Trainers who apply that same automation mindset to GLP-1 client management are the ones who can serve this population profitably at scale.
For the broader operational framework on managing larger client rosters with automation, see our guide on building a sustainable personal training business.
GLP-1 Coaching as a Business Opportunity
The market reality is straightforward: about 1 in 8 US adults are on GLP-1 medications (KFF, 2025), and the number is growing. The oral GLP-1 pill launch in January 2026 further expanded access beyond injectable-only populations. This is a structural shift, not a temporary trend.
The professional gap is the business opportunity. NASM's survey found 50% of trainers working with GLP-1 clients report "skinny fat" outcomes. Half the trainers currently serving this population deliver suboptimal results because they lack specialized programming and tracking systems.
A trainer who can demonstrate evidence-based GLP-1 programming expertise, body composition tracking methodology, and structured client workflows has a service most competitors cannot match:
Pricing premium: GLP-1 coaching as a specialized service tier can support 20-40% premium pricing above standard coaching rates, justified by specialized knowledge and tracking intensity
Credential pathway: ISSA launched a dedicated GLP-1 Weight Loss Support Training certification in 2025, validating the specialization and providing an accessible credential for trainers who want to formalize their positioning
Retention advantage: GLP-1 clients who see body composition improvements (not just scale changes) through your programming have a data-driven reason to stay -- unlike clients whose only metric is a number medication alone can deliver
Key Takeaways
The muscle loss risk is real and quantifiable: Up to 40% of weight lost on GLP-1s can be lean mass without resistance training. Trainers are the lean mass preservation specialists in the GLP-1 care model.
Standard intake forms are not enough: GLP-1 clients require medication-specific assessment fields covering dosage, titration schedule, side effect profile, protein intake, and body composition baselines.
Programming specificity matters: 65-85% 1RM, 2-4 sets of compound movements, 3-4 sessions per week, 48-72 hours recovery. Three phases (Foundation, Progressive Overload, Strength-Focused Preservation) map to the GLP-1 treatment timeline.
Autoregulation is non-negotiable: RPE-based intensity management accounts for the variable energy reality of GLP-1 therapy. Reduce load on bad days rather than skipping sessions.
Protein is the most actionable nutrition lever: 1.6-2.2 g/kg body weight daily, distributed across meals. Most GLP-1 clients are significantly under target.
Track body composition, not just weight: Monthly BIA, relative strength benchmarks, grip strength, and protein compliance. Escalate if lean mass loss exceeds 25% of total weight lost.
Technology enables scale: Automated check-ins, dashboards, and alert thresholds let you manage a GLP-1 roster without manual outreach for every client every week.
Ready to build your GLP-1 coaching practice? Download the GLP-1 Client Intake & Autoregulation Template -- the complete PDF includes all assessment fields, strength baselines, protein compliance tracker, and a FitFlow-importable check-in file. Free for FitFlow members.
Consult a healthcare professional before starting any new exercise or nutrition program. This guide provides a fitness programming framework, not medical advice. Results vary by client, medication type, dosage, and training history. FitFlow is our product. References to other platforms and research are based on publicly available information as of March 2026.
Frequently Asked Questions
Comments