Programming Around Chronic Pain: A Decision Tree for Online Coaches
Your client just texted you that their knee felt off again. Same knee, same Monday, same flare that crept in six weeks ago and never fully cleared. You have ninety seconds before you reply.
Most coaches' next move is the wrong one.
The default reply, "let's pull squats this week, swap in leg press, see how you feel," costs you retention. It costs your client load. And it quietly installs a fragile-identity script that lasts longer than the flare itself. Here's the thing: the evidence does not support the default. The 2018 Lancet low-back-pain series flatly states that rest is not the right intervention for most chronic musculoskeletal pain. Cochrane reviews say exercise. The 2024–2025 BJSM editorial series says stop framing pain as damage and start framing it as a load-management decision.
But you are an online coach with thirty clients, not a physiotherapist. Three of your clients have some pain modifier this week. Your check-in window is twenty minutes. You need a paste-into-Monday-morning protocol, not a pain-neuroscience seminar.
This is that protocol. The 4-factor decision tree, the 9 modifiable variables, and the phase-aligned modification map I run on every pain-presenting client in my roster. If you want the full operational artifact (the decision tree as a one-pager, the irritability self-test, the red-flag screening checklist, and the roster pain-triage map), grab the Pain-Modification Decision Guide here. It is built for paste-into-your-check-in-template use.
One thing before any of it: this post is education for personal trainers and coaches working in the on-program scope of practice. It is not a substitute for clinical assessment. The red-flag screening criteria in Section 5 are non-negotiable. When they fire, you refer out. We will get there.
The framework starts with what the science actually says.
What the Pain Science Actually Says (And What It Doesn't)
The single most important reframe in modern pain science is this: pain and tissue damage are not the same thing.
That sentence sounds like a hot take. It is not. It is the consensus position of the International Association for the Study of Pain, the British Journal of Sports Medicine editorial board, the authors of the Lancet 2018 low-back-pain series, and the practitioner-academics (Moseley, Butler, Lewis, O'Sullivan, Caneiro, Lehman) whose work has shifted how clinicians approach persistent musculoskeletal pain over the last fifteen years. Pain is a protective output of the brain. It integrates many inputs. Tissue state is one of them, but so are sleep, stress, prior experience with the same pattern, threat appraisal, and context. A bulging disc on an MRI does not predict back pain. A chronic tendinopathy on imaging does not predict tendon pain.
This matters for your roster because the standard coaching response (your back hurts, so your back must be damaged, so we stop loading your back) gets the causal chain wrong. The pain is real. The damage framing is usually not.
The 3-mechanism classification
The most useful clinical framework you can carry as an online coach is the mechanism-based pain classification from Smart and colleagues (2012, 2014). It groups musculoskeletal pain into three categories. You are not diagnosing. You are noticing the pattern so you can route correctly.
Nociceptive pain is tissue-driven. It reliably reproduces with a specific movement, load, or range of motion. Squat to depth, pain. Avoid the bottom range, no pain. This is the most coach-modifiable category.
Peripheral neuropathic pain is nerve-driven. It follows a dermatomal pattern (a stripe of skin innervated by a specific spinal nerve), often presents as burning or sharp, and frequently includes numbness, tingling, or weakness. This is almost always a refer-out trigger in coaching scope.
Nociplastic pain is what the field used to call "central sensitization." The mechanism is the nervous system's gain turned up. Pain that does not track cleanly with mechanical inputs, often has high context modifiers (stress, sleep, time of day), often widespread. Graded exposure and reassurance beat deload here. So does honoring sleep and stress as variables.
If you can place a client's pain in one of these three boxes, and you usually can after one or two check-ins, you have the input the decision tree in Section 5 wants.
The Cook & Purdam tendinopathy continuum
For tendons specifically, Cook and Purdam (BJSM, 2009, revisited 2016) gave us the continuum model: reactive, dysrepair, degenerative. The stage matters because each stage responds best to a different loading strategy.
Reactive tendons are fresh from a load spike. They want isometric loading and they do not want eccentric volume. Rio's 2015 and 2017 protocols (five sets of forty-five seconds at approximately seventy percent maximal voluntary contraction) are the best-evidenced analgesic intervention we have for the reactive phase.
Dysrepair tendons sit between reactive and degenerative. They tolerate moderate loading with progressive overload. Heavy slow resistance protocols (Beyer et al. 2015) show comparable outcomes to traditional eccentric programs with better adherence.
Degenerative tendons are the long-standing ones. Tissue is remodeled and structurally different from a healthy tendon. They respond well to heavy slow resistance and consistent loading. They do not respond well to extended rest.
Notice what the continuum is not telling you. It is not telling you to deload. At every stage, the answer involves loading. The question is which loading shape.
The Lancet low-back-pain consensus
The 2018 Lancet series on low back pain (Hartvigsen et al.) made the position explicit: for chronic non-specific low back pain, exercise is the recommended intervention and rest is not. The 2024 and 2025 Cochrane reviews on exercise therapy for chronic low back pain reinforce this with updated effect sizes. The Lewis & O'Sullivan BJSM 2018 editorial ("Is it time to reframe how we care for people with non-traumatic musculoskeletal pain?") pulled the threads together into the operational reframe that practitioner-academics have built on since.
The ACSM 2026 Position Stand (Currier et al., MSSE 58(4)) is scoped to healthy adults rather than chronic-pain populations, but its core message squares with the load-management framing in your roster: any structured resistance training meaningfully improves muscle function and physical performance, and individualizing programs to increase participation matters more than tight adherence to specific prescription variables. Read it alongside Hartvigsen and Hayden, not in their place.
What this reframe does not say
The reframe does not say always train through pain. It does not say pain is just in your head. It does not say deload is never the answer. There are presentations where pull-back or refer-out is the right move. The next four sections give you the operational rules for telling them apart.
The Coaching Reality: Why "Back Off" Is the Default and Why It Costs You
The deload default is not stupid. It feels conservative. It is what most coaching education teaches. It is the lowest-risk move for the coach. Three reasons coaches reach for it first.
Reason one: liability anxiety. We are not physiotherapists, and the fear of "what if I tell them to train through this and it gets worse" is real. The certification bodies (NSCA, ACSM, NASM, ACE) do not give you a decision tree for pain modification. They give you a scope-of-practice line and a "refer to a qualified professional" recommendation.
Reason two: no framework. Coaching education jumps from program design to recovery to deload weeks without ever giving you the operational vocabulary for pain-mediated modification. If your only tools are "load it" and "rest it," everything that hurts looks like a rest problem.
Reason three: async coaching makes assessment harder. You cannot palpate a tendon over Trainerize. You cannot watch the client warm up. You read a text and decide. The conservative move feels like the right default when assessment is bandwidth-limited.
But the default has a cost, and I have watched it play out the same way more times than I want to admit. Four clients in a row, three-week deloads, ten percent off the best-set load, gone within ninety days. The retention data backs this up. PTDC and OPEX 2024 practitioner surveys both report higher 90-day churn for clients who experience deload phases longer than two weeks. The strength cost is documented: five to fifteen percent drops on substituted movements after two weeks off the primary pattern, with longer recovery curves the older the lifter. And there is a psychological cost that does not show up in any retention dashboard. The "I'm fragile" identity quietly installs after the second or third deload-and-modify cycle. Clients start negotiating their training around fear of flare rather than progression toward goals.
Pulling out of Trainerize for three weeks because of a low-irritability mechanical knee tweak is over-prescription. It might be the most overprescribed coaching intervention in the field. The framework in the rest of this post is built to give you a more accurate move at the moment your client texts you.
The 4 Failure Modes Coaches Make on Pain-Presenting Clients
Before the decision tree, name the failure modes the tree is designed to prevent. There are four. Two are symmetric (over- and under-protection). Two are about scope.
Failure mode 1: Overprotection. You default to deload when modification was the right answer. Symptoms are low-irritability and mechanically reproducible. The client could have continued the movement with a load reduction or a tempo change. Instead you pulled the movement. The client loses load on the substitute, loses confidence in the original pattern, and is now seven days into a three-week deload that did not need to happen. This is the most common failure mode by far.
Failure mode 2: Underprotection. You train through when pull-back was the right answer. Symptoms are high-irritability or red-flag-suspected. You said "push through, see how it feels" and the irritability climbed across three sessions. Now the presentation is worse than when you started, the client is losing trust in your coaching, and the protocol you should have run on Day 1 (isometrics, deload, or refer out) has now lost two weeks of intervention time. Less common than overprotection but more costly when it happens.
Failure mode 3: Scope creep. You attempt to diagnose mechanism or treat clinically. "Sounds like patellar tendinopathy, let me put you on the Rio protocol" without verifying mechanism, irritability, or whether a clinical assessment has happened. This is a legal and ethical exposure. Even if you are right about the mechanism, the framing is wrong. You are coaching the modification, not diagnosing the pathology. The language matters. So does the work.
Failure mode 4: Scope avoidance. The mirror of scope creep. You refer out reflexively the moment any client says "ow," even when the presentation is non-acute, non-red-flag, mechanically modifiable. The client loses time. The physio appointment confirms what you could have addressed in the program (irritated tendon, modifiable loading) and the client is out of pocket for an unnecessary visit. Trust in your coaching erodes because you handed off rather than coached. Amanda, the trainer in her first ten clients, does this most often. It is correctable.
The decision tree below routes around all four. The four factors it uses are the inputs that distinguish each failure mode from a correct call.
The 4-Factor Pain-Modification Decision Tree
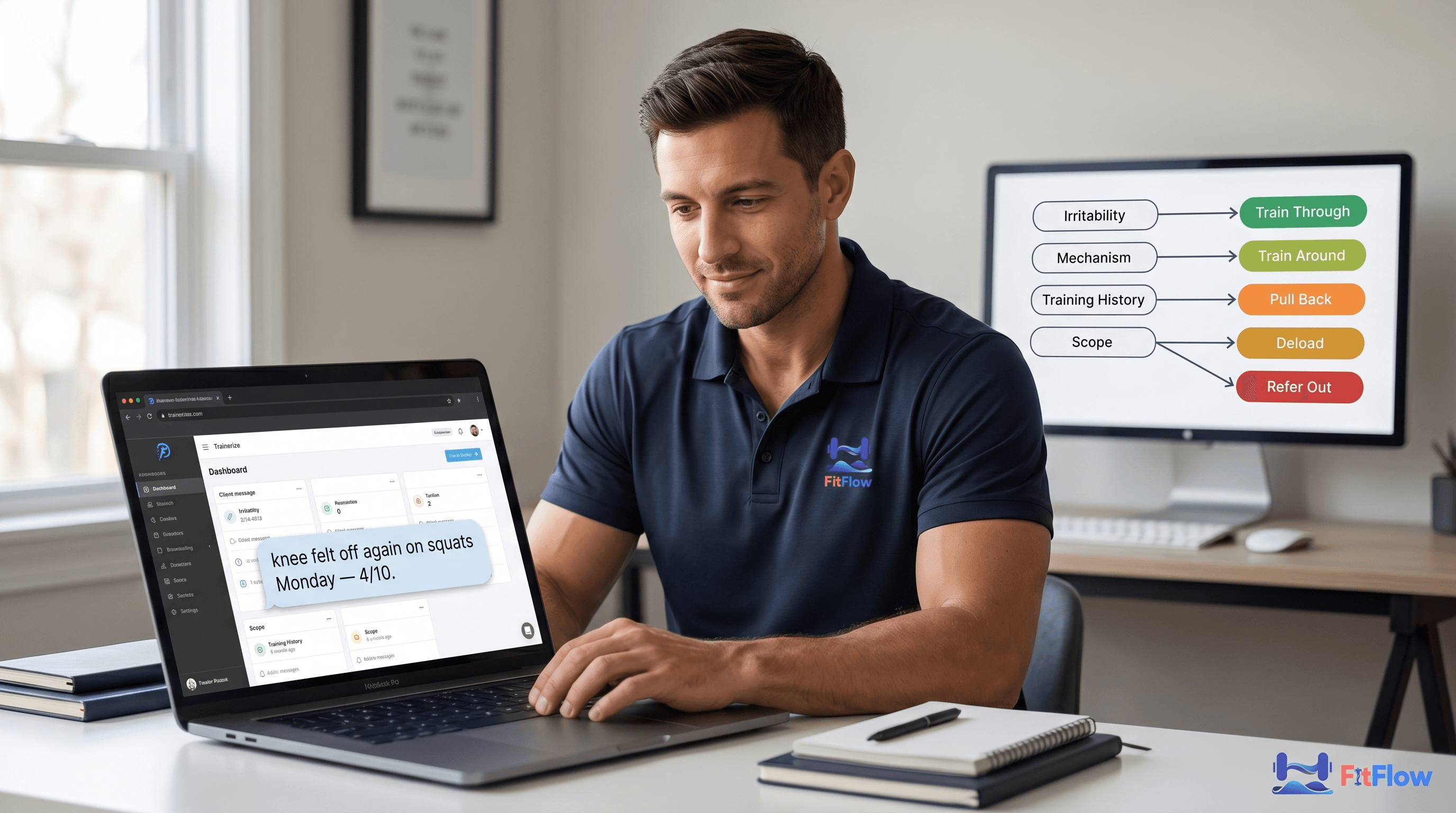
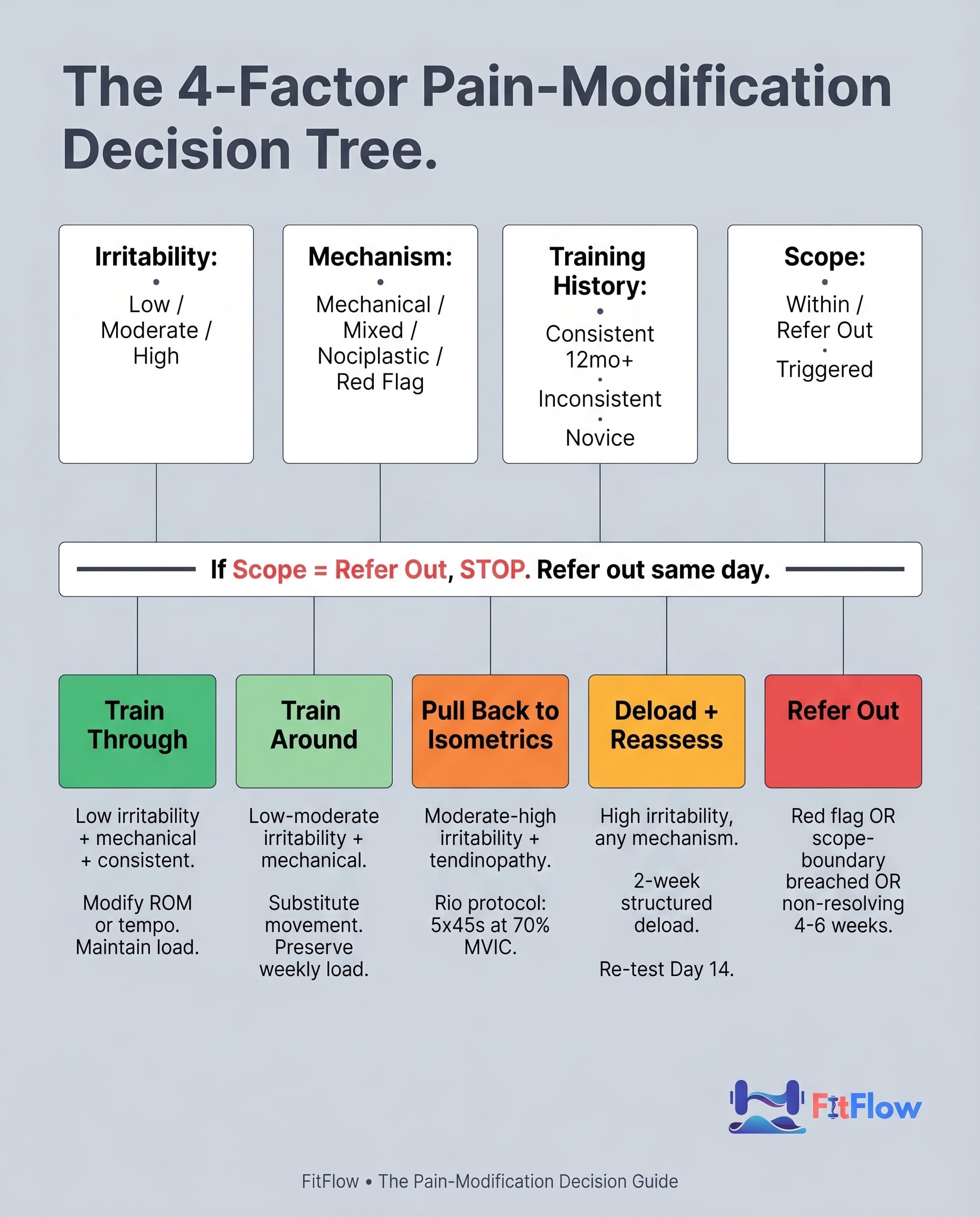
The tree has four inputs. Run them in this order: scope flags first (because they short-circuit everything else), then irritability, then mechanism, then training history.
Factor 1 — Scope flags (the short-circuit)
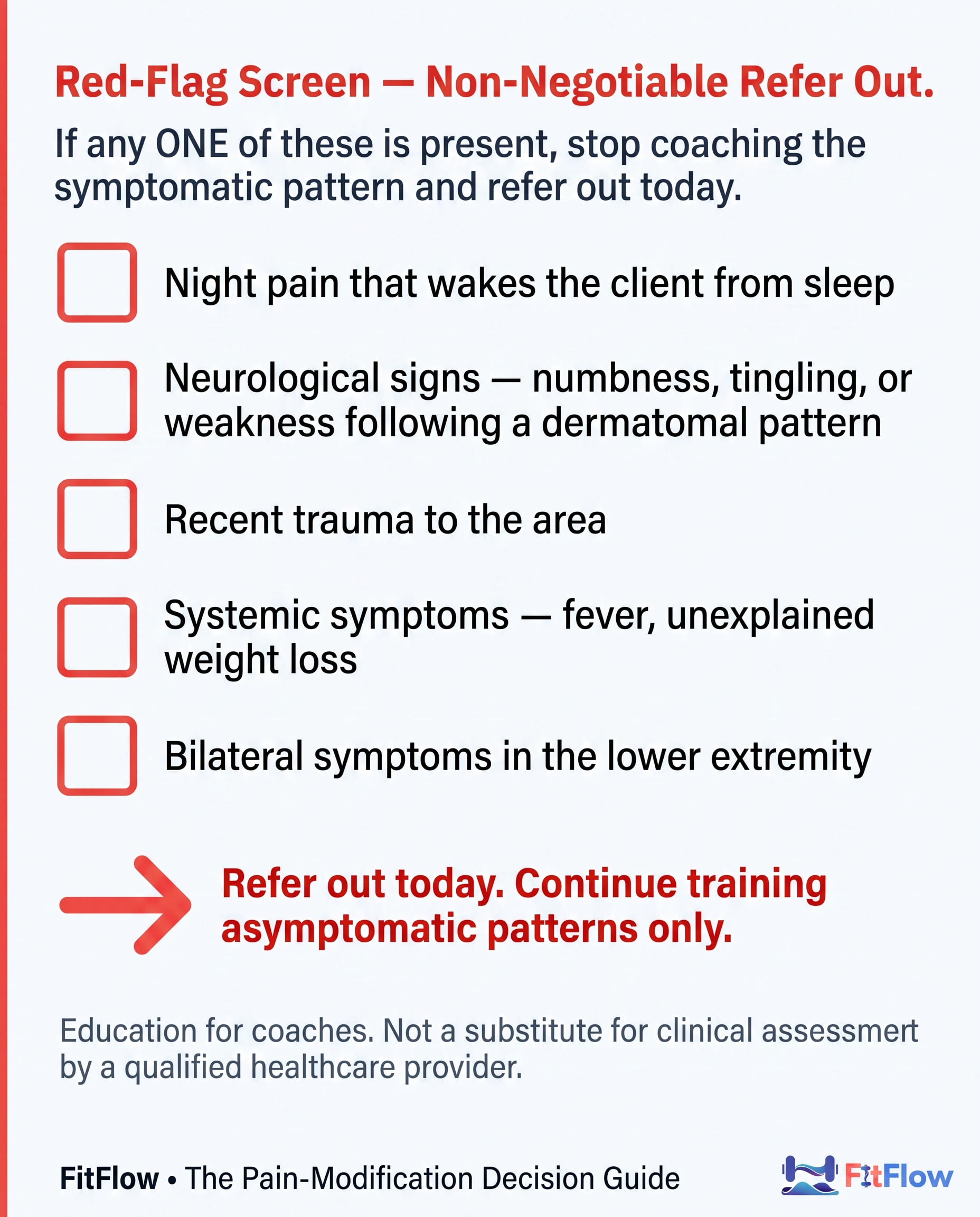
If any of the following are reported, stop running the tree and refer out the same day. These are the red-flag screening criteria for the coaching context, adapted from the standard clinical red-flag list and simplified for coach-facing use.
Red-flag screen: night pain that wakes the client from sleep; neurological signs (numbness, tingling, or weakness following a dermatomal pattern); recent trauma; systemic symptoms (fever, unexplained weight loss); bilateral symptoms in the lower extremity. If any one is present, you stop coaching the symptomatic pattern and refer out today. Non-negotiable.
Refer out is also the right move when (a) the client requests clinical assessment, or (b) a high-irritability presentation has not resolved with structured modification across four to six weeks. Refer-out is a safety net, not avoidance.
If the red-flag screen is clean, continue.
Factor 2 — Irritability tier
Irritability is the most diagnostic input you have. It tells you how reactive the tissue is right now. Use a three-question self-test (the same one in the Decision Guide):
How quickly does the symptom appear during training? (Onset)
How intense is the symptom at its peak? (Intensity, 0–10)
How long does the symptom take to settle? (Recovery)
Bucket:
Low irritability: symptom onset >20 min into the session, intensity ≤3/10, recovery same-day or within a few hours.
Moderate irritability: onset in the first 10 min, intensity 4–6/10, recovery within 24 hours.
High irritability: onset on warm-up or in the morning, intensity 7+/10, recovery >24 hours or sleep-disturbing.
Factor 3 — Mechanism (carry forward from Section 2)
Place the presentation in one of the three boxes from Section 2: nociceptive (mechanical-reproducible), nociplastic (poor mechanical reproducibility, high context modifiers), or mixed. Peripheral neuropathic presentations are caught by the scope-flag screen above.
Factor 4 — Training history
Is the client consistent-trained for twelve months or longer, or inconsistent / novice / detrained? Tissue tolerance is a function of training history. A consistent-trained client with low-irritability nociceptive pain has more headroom for in-pattern modification than a detrained client with the same presentation, who often benefits from a brief pull-back even at low irritability.
Outputs — pick one branch
Once you have the four inputs, the tree routes to one of five branches. Each has a paste-into-the-session-note prescription template.
Branch A — Train Through (load-tolerated). Low irritability + mechanical (nociceptive) + consistent-trained + within scope. The movement stays. You modify ROM or tempo only. Example prescription: "Back squat to 3/10 pain ceiling, pause-tempo 3-1-X-1, depth set by pain-free range. Drop 10% load. Track in check-in: onset minute, peak intensity, next-day status."
Branch B — Train Around. Low-moderate irritability + mechanical + any history + within scope. You substitute the irritated movement pattern. Total weekly load is preserved through accessory volume and isometrics on the irritated pattern. Example prescription: "Replace back squat with belt squat or split squat for three weeks. Add patellar tendon isometric work twice per week: Spanish squat 5 × 45s at 70% effort. Reassess Day 14."
Branch C — Pull Back to Isometrics. Moderate-to-high irritability + tendinopathy mechanism + any history + within scope. Run the Rio protocol: five sets of forty-five seconds at approximately seventy percent MVIC, two minutes rest, twice per day for one to two weeks. Combine with reduced (not eliminated) primary-pattern volume; target sixty percent of the prior block's volume. Reassess weekly. Example prescription: "Spanish squat isometric, 5 × 45s @ 70% effort, 2 min rest, 2× per day. Concurrent reduced squat volume at 60% of prior block. Reassess Day 7 with the irritability self-test."
Branch D — Deload + Reassess. High irritability + any mechanism + within scope. Run a two-week structured deload: fifty percent volume, eighty percent intensity of the recent block, explicit re-test markers at Day 14. The deload is not "rest." It is loaded reduction. Example prescription: "Drop squat-pattern volume to 50%, intensity to 80%, for 14 days. Concurrent isometric work daily. Re-test Day 15 with full warm-up + irritability self-test. Decision point: return to full block if score ≤10/30, extend deload if score 11–20, escalate if >20."
Branch E — Refer Out. Red-flag screen fires OR scope-boundary breached OR client request OR non-resolving after four to six weeks of structured modification. Example prescription: "Refer to [physiotherapist/sports medicine MD]. Pause all symptomatic-pattern work pending clearance. Continue upper-body / asymptomatic-pattern training in the meantime. Document referral in check-in notes."
Five branches. Each with a concrete prescription. The four factors route you. If the tree returns an output that feels wrong on a specific client, check three things: did the scope flags get an honest answer, did irritability bucketing match the client's actual report, and is the mechanism classification confident or guessed? Usually one of those three is the source of the disagreement.
The full tree, with a printable flowchart and three worked examples, is in the Pain-Modification Decision Guide.
The Modifiable Variables Menu — 9 Levers Before You Deload
The tree's "Train Through" and "Train Around" branches both produce prescriptions that adjust specific training variables. The menu below is the operational list of what to adjust, in reach-first order. Most coaches reach for variable number seven first. Reach for variable number one first instead.
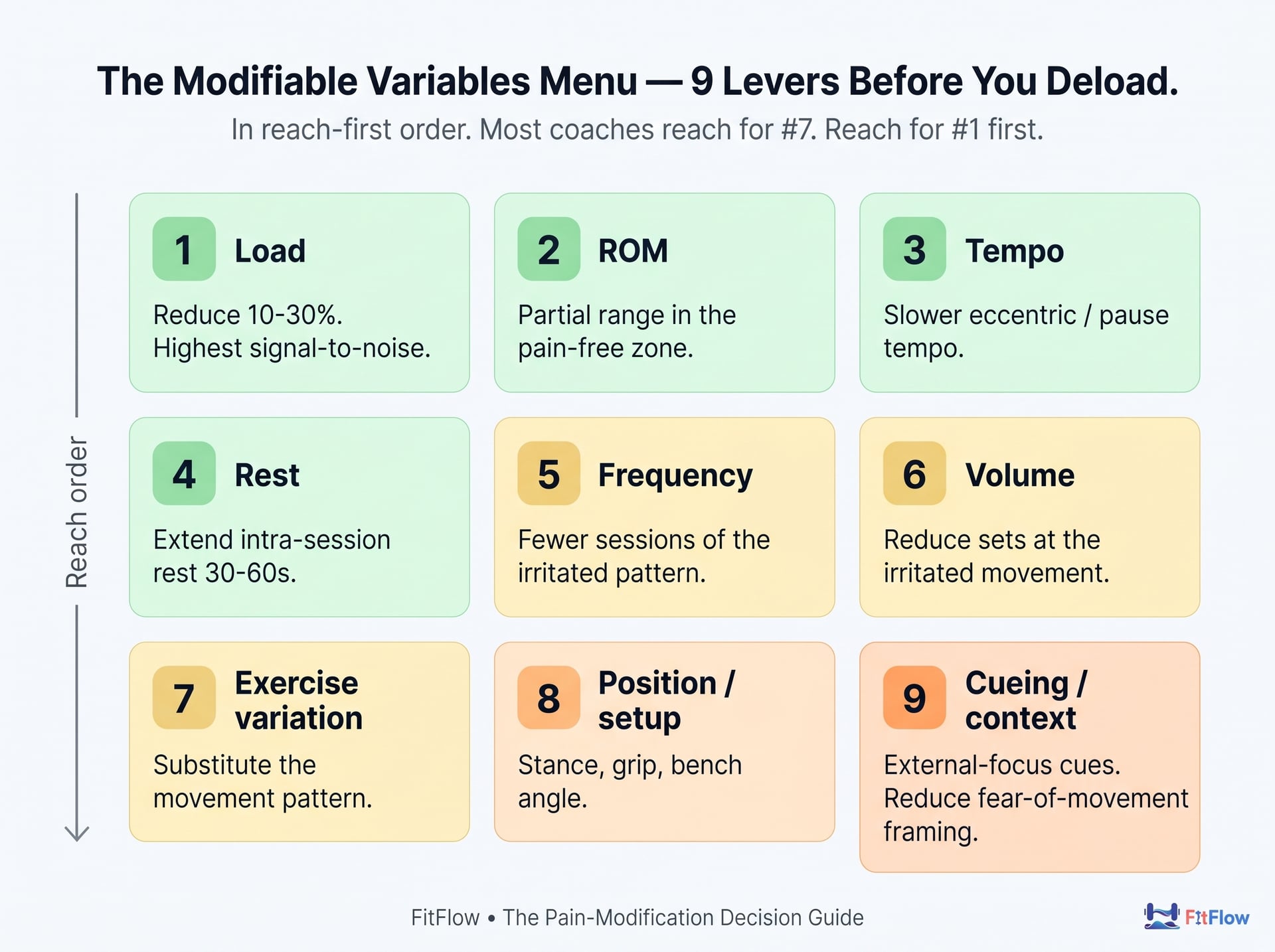
Load. A reduction in the ten-to-thirty-percent range is the most common adjustment. It is the variable with the highest signal-to-noise: if a low-irritability mechanical presentation does not respond to a fifteen-percent load cut within two sessions, the framing is probably wrong. The presentation is not what you thought it was, or there is a context modifier you missed. Reach here first.
Range of motion. Partial ROM in the pain-free zone is the second-most-common adjustment. The classic example: box squat to a two-inch-higher box for a knee presentation; floor press for a shoulder presentation. ROM is a precision lever. You are saying "yes to loading, no to the specific range that's reactive."
Tempo. Pause-tempo, slower eccentrics, or controlled concentrics reduce peak force at the irritable position without reducing total work. Useful for tendinopathy presentations where the peak-force moment is the irritation moment. Three-second eccentric, one-second pause, explosive concentric is the canonical pattern for reactive tendons.
Rest. Extending intra-session rest by thirty to sixty seconds reduces accumulated fatigue without changing load or volume directly. Especially useful for late-set irritation that climbs across the session.
Frequency. Reduce sessions per week of the irritated pattern; preserve weekly total via other movements. From three squat sessions to two, with the third becoming a single-leg accessory day, for example.
Volume. Reduce sets at the irritated movement; maintain total via accessories. Three sets of squats become two sets of squats plus three sets of split squats.
Exercise variation. This is the canonical "train around." Substitute the movement pattern. Back squat to safety-bar squat, conventional deadlift to hex-bar, flat bench to incline. A useful late-reach lever, not a first-reach lever.
Position / setup. Stance width, grip width, bench angle, foot position on the leg press. These are often the cheapest interventions. You change one setup variable and the symptom resolves at the same load.
Cueing and context. This one matters more than coaches expect. External-focus cueing ("press the floor away") reduces movement anxiety compared to internal-focus cueing ("contract your quads"). Reducing fear-of-movement cueing, and explicitly framing pain as a protective output rather than a damage signal, is part of the prescription. This is not "in your head" coaching. It is using the inputs to the protective output that are within your scope.
The reach order is not arbitrary. It follows a principle: change the variable closest to the irritability driver first. Load and ROM are closest to the immediate mechanical input. Substitution and cueing are furthest. Reaching for substitution first is the deload-default in disguise. You have removed the movement rather than adjusted it.
The 80/20 of training results post lays out the high-level lever ranking for asymptomatic clients; the menu above is its pain-domain instantiation. Both apply.
Phase-Aligned Modification Map
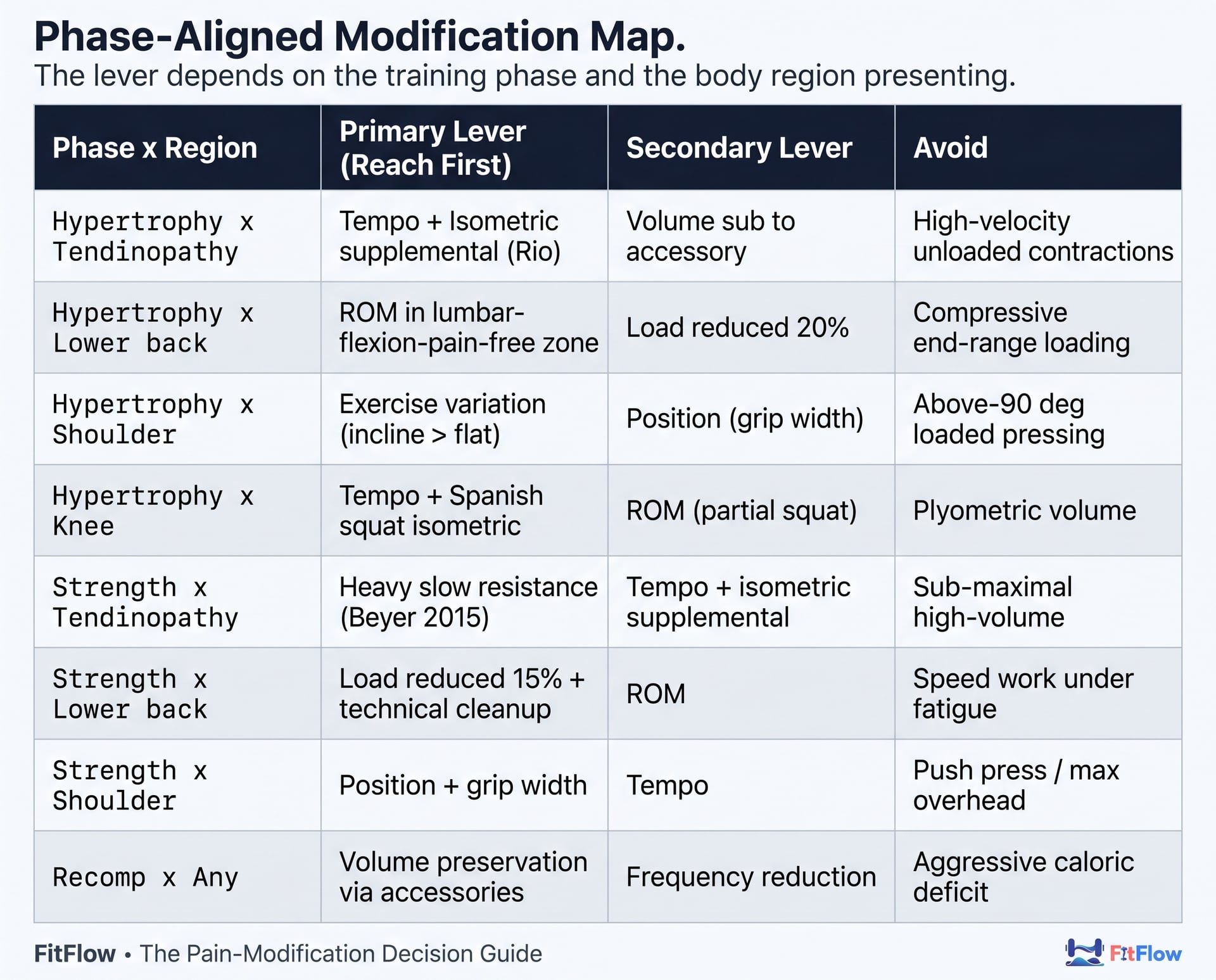
The lever you reach for first changes with the client's training phase and the body region presenting. The matrix below is the cheat sheet. The full version, with 12 rows including specific exercise substitutions, is in the Decision Guide.
Phase × Region | Primary lever (reach first) | Secondary lever | Avoid in the symptomatic phase |
|---|---|---|---|
Hypertrophy × Tendinopathy (any) | Tempo + Isometric supplemental (Rio) | Volume substitution to accessory | High-velocity unloaded contractions |
Hypertrophy × Lower back | ROM in lumbar-flexion-pain-free zone | Load reduced 20% | Compressive end-range loading (e.g., wide-stance heavy front squats) |
Hypertrophy × Shoulder | Exercise variation (incline > flat; landmine > overhead) | Position (grip width) | Above-90° loaded pressing if symptomatic |
Hypertrophy × Knee (patellar/quad) | Tempo + Spanish squat isometric | ROM (partial squat to higher box) | Plyometric volume |
Strength × Tendinopathy (any) | Heavy slow resistance (Beyer 2015) | Tempo + isometric supplemental | Sub-maximal high-volume contractions |
Strength × Lower back | Load reduced 15% + technical cleanup | ROM in pain-free zone | Speed work under fatigue |
Strength × Shoulder | Position + grip width; consider press substitution | Tempo | Push press / max-effort overhead if symptomatic |
Recomp × Any presentation | Volume preservation via accessories; deload primary | Frequency reduction | Aggressive caloric deficit during high-irritability windows |
The matrix is a starting point, not an algorithm. The 4-factor tree gates which row applies; the matrix tells you which lever to reach for once the row is selected. A novice client in a recomp phase with a moderate-irritability shoulder presentation does not get the same prescription as a consistent-trained client in a strength phase with the same shoulder presentation. The training-history factor (Factor 4) modifies the matrix's output.
Two-Client Case Study: Same Body Region, Different Prescriptions
The cleanest test of a decision framework is whether it produces different prescriptions for clients who present similarly on the surface. These two clients both walked in with low-back complaints. The protocols are different. The outcomes are different. The framework is the same.
Case A — Mechanical low back, train around
Thirty-two-year-old male, four years of consistent training, lifts four days per week. Texted: "Tweaked my back on deadlift Monday. Same spot, right side, low. 4 out of 10 during, gone the next day, fine on squat. Don't want to take a week off."
Run the tree. Scope flags: clean (no night pain, no neurological signs, no trauma). Irritability: low. Onset during the lift, peak 4/10, same-day recovery. Mechanism: mechanical, with clean reproducibility (symptom on conventional deadlift, no symptom on hex-bar). Training history: consistent-trained.
Tree output: Branch B (Train Around).
Prescription: replace conventional deadlift with hex-bar for three weeks. Maintain rep ranges and volume. Add a posterior-chain accessory: single-leg RDL for two sets twice per week. Reassess Day 14.
Day 14: symptom present zero of seven training days. Conventional deadlift reintroduced at ninety percent of prior block, no symptom. Day 30: full block load restored. Client describes the modification as "the most useful two weeks of training I've had in six months" because nothing was paused.
Case B — Nociplastic low back, graded exposure
Forty-one-year-old female, eighteen months of inconsistent training (work stress disruptive in 2025). Texted: "My back's been weird all week. Hurts on Monday but not Tuesday. Fine in the deadlift on some days, sore for hours on other days. Not sure what's going on."
Run the tree. Scope flags: clean. Irritability: moderate (intensity 4–6/10 on flare days, recovery within 24h). Mechanism: nociplastic-leaning, with poor mechanical reproducibility and high context modifiers (the inconsistency is itself a signal). Training history: inconsistent.
Tree output: Branch B (Train Around) with a graded-exposure overlay and explicit nociplastic-management additions.
Prescription: substitute hex-bar for conventional deadlift for three weeks (the same lever as Case A). Lift only on days when the irritability self-test totals 6/30 or below (the "low" tier). On flare days, hold load and reduce volume rather than skip the session entirely. Add walking on rest days (the off-tissue side; see Why Your Clients Are Not Recovering). Reassure: pain ≠ damage. The script the client recites before sessions is "my back is sore, my back is not injured, and loading is the right intervention right now."
Day 14: symptom-free training days = three of seven (up from zero of seven the prior month). Day 30: conventional deadlift restored. Client now self-administers the irritability self-test during the warm-up.
The lesson is the section's title. Same body region. Different mechanisms. Different prescriptions. Same framework. The deload default would have given both clients the same prescription, a week off, and would have produced worse outcomes for both. The framework's value is the differentiation, not the formula.
Week-1-to-Week-8 Implementation: Convert This Into Your Roster's Templates
The framework lives or dies in your operational templates. Here is the eight-week rollout.
Week 1: add one field to your intake form. "Do you currently have any pain that modifies your training? If yes, briefly describe: location, when it started, what makes it worse, what makes it better." Two sentences. That is the screening at the front door.
Week 2: add the irritability self-test (three questions, scoring 0–30) to your weekly check-in template. Every client fills it out every week. Asymptomatic clients score zero in five seconds. Pain-presenting clients give you the data you need to bucket irritability without an extra video call.
Week 3: pilot the 4-factor tree on one currently pain-presenting client. Document the branch you picked, the prescription you wrote, and the reasoning. Save it as the first entry in your pain-modification log.
Weeks 4–6: roll out across all pain-presenting clients. Add two more cases to the log. Pay attention to the cases where the tree's output disagrees with your intuition. Those are the cases that teach you whether the framework or the intuition needs updating.
Weeks 7–8: review the log. You should have five to eight documented cases. You should see your refer-out rate decrease (because scope clarity is rising) and your overprotection rate decrease (because the tree is doing the routing your default used to do). This is the same operational discipline that drives the rest of the Online Coaches 30-Client Wall Operations Playbook.
By Week 8, the pain-modification framework is part of your roster's standard operating procedure. New pain presentations get triaged the same way new strength plateaus do. There is a defined process, and the bandwidth cost per case drops.
Closing — The Operational Move + Scope Boundary
Pain is a load-management problem, not a damage problem, in most of the presentations you will see on your roster. The 4-factor decision tree gives you the framework to act on that fact. The modifiable-variables menu gives you the variables to adjust. The phase-aligned matrix gives you the starting prescription. The two case studies show you that same-region presentations can need different protocols. The eight-week rollout converts the framework into your roster's standard operating procedure.

If you want the framework in operational form (the decision tree as a one-page flowchart, the irritability self-test as a printable, the red-flag screening checklist, the four common-presentation mini-protocols for patellar, low back, shoulder, lateral elbow, and the Roster Pain-Triage Map), download the Pain-Modification Decision Guide here. It is built for paste-into-your-check-in-template use.
Sister posts:
Why Your Clients Are Not Recovering: the off-tissue / off-program variable diagnostic. This post is the on-tissue side.
Online Coaches 30-Client Wall Operations Playbook: the operations playbook this pain-modification protocol slots into as one of seven named systems.
Evidence-Based Program Design: the foundation parent.
Progressive Overload Misunderstood: load progression is the asymptomatic-state mechanism; this post is the symptomatic-state modification.
What Elite Coaches Do Differently: the meta-decision triage parent.
The 80/20 of Training Results: the high-level lever ranking that frames the modifiable-variables menu.
Improve Results Without Changing Training: the off-program variable hierarchy sister.
Why Most Hypertrophy Programs Fail After 6 Weeks: physiology-stagnation is the asymptomatic failure mode; pain is the symptomatic one.
Recovery as a Growth Lever: systemic recovery is the off-tissue side of load tolerance; this post is the on-tissue side.
Scope-of-practice boundary. This post is education for personal trainers and coaches working with clients in the on-program scope of practice. It is not a substitute for clinical assessment by a qualified physiotherapist, sports medicine physician, or other healthcare provider. If your client presents with any of the red-flag screening criteria in Section 5, or if you are unsure whether a presentation falls within your scope, refer out the same day. Refer-out is not avoidance. It is the right move when the criteria are met. The framework in this post raises the floor of your routing accuracy. It does not raise your scope.
Frequently Asked Questions
Comments