Tempo Work for Hypertrophy: When It Matters, When It Doesn't
Pull up any five program templates from your roster right now. Count how many have a tempo column. For each program that has one, answer this out loud: "For this client, on this exercise, why did I prescribe a 3-1-1-0 cadence and not 4-0-2-0 or self-selected?"
If you can defend the prescription with a specific reason (a tendinopathy protocol, an eccentric-overload block, a novice in week six, a lengthened-partial cue for a lagging muscle), you're in the 20% of coaches using tempo correctly. If you're hedging with "it's just what the template has" or "tempo creates more time under tension and TUT drives hypertrophy," you're prescribing theater. Theater on a 30-client remote roster bleeds compliance and produces zero hypertrophy advantage the evidence can actually measure.
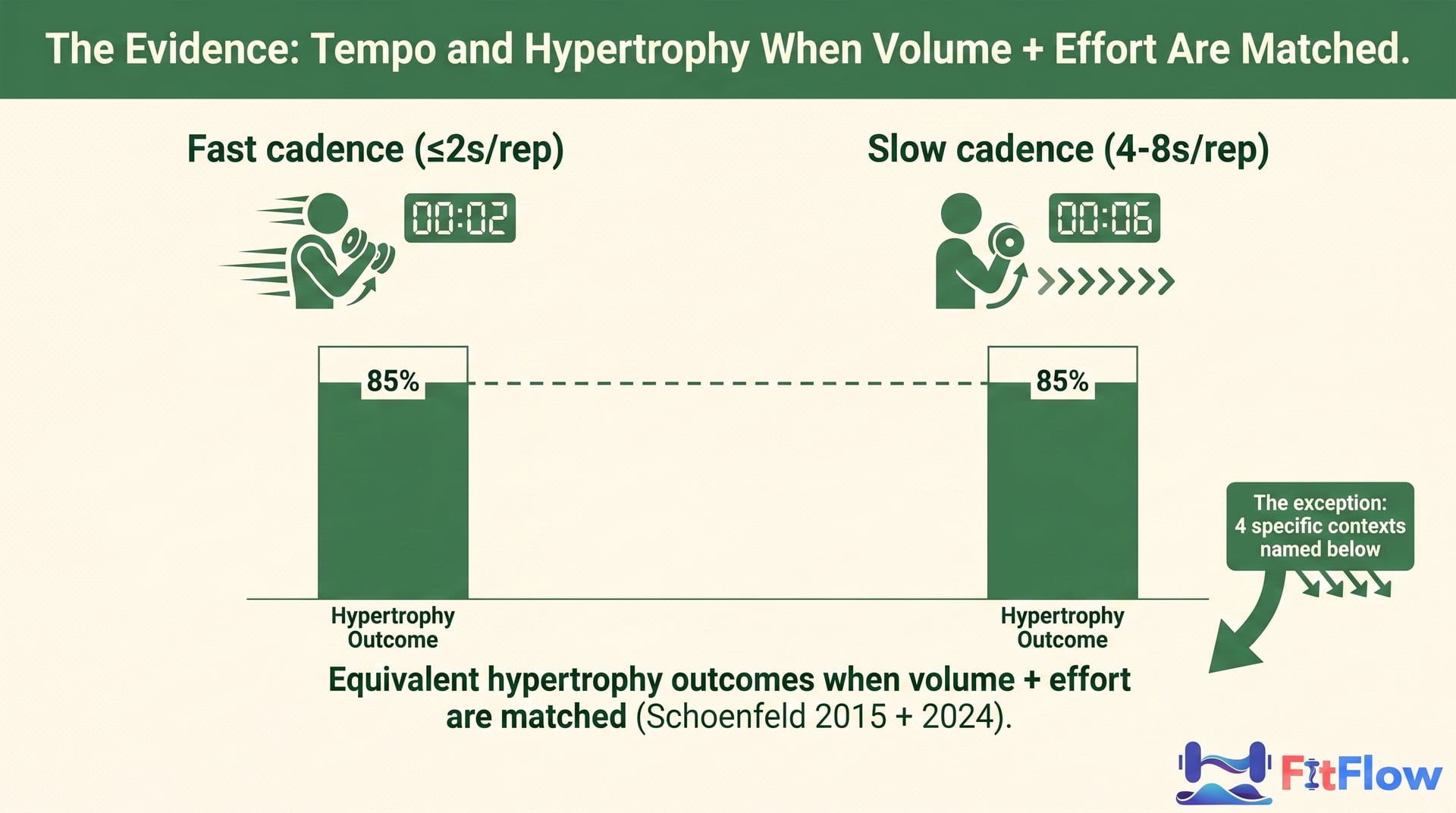
Here's the part most articles dance around: tempo prescription is the most over-prescribed, under-evidenced variable in modern hypertrophy programming. For 70–80% of general-population hypertrophy clients you're coaching this week, training 2–5x weekly in the 5–30 rep range, the tempo column on the program is decorative. Schoenfeld's 2015 meta-analysis and the 2024 ROM/tempo update both land in the same place: when volume and effort are matched, fast versus slow cadence produces equivalent hypertrophy outcomes. Tempo matters in four specific, defensible contexts. So the operational move is to know those four contexts, prescribe surgically inside them, and stop bleeding client compliance in the 80% where tempo does nothing.
Skip ahead → The 4-Context Tempo Decision Tree (free download)
This article gives you the evidence, the four contexts with citation density per branch, the decision tree, the roster-segmentation table, the program-note templates, and the 5-step audit to clean up your existing templates this week. By the time you finish, you'll have a defensible answer for every tempo column on every program, including the columns you delete.
1. Why the tempo column persists in your templates (and where it came from)
The tempo column on your client's program has a history, and that history explains why it sticks around despite a decade of evidence that should have removed it.
Through the late 1980s and 1990s, "Time Under Tension" became a working framework in bodybuilding programming. Mike Mentzer, Fred Hatfield, and the early hypertrophy theorists turned observations from elite bodybuilders into prescriptive protocols. The reasoning was plausible for its era: if muscle fibers experience longer tension, metabolic stress and mechanical loading accumulate to higher levels, and that accumulation should drive greater adaptation. The hypothesis was fine. Writing specific second-by-second tempos into every set of every program was a stretch the underlying physiology never asked for.
The Wilk et al. 1993 super-slow study is the citation many trainers still reach for when defending tempo prescription. Read that paper today and what should have been obvious at the time jumps out: the protocol was single-joint, the subjects were advanced lifters, volume wasn't effort-matched, and the practical implications got extrapolated far beyond what the methodology supported. Citing Wilk 1993 to claim "slow tempo drives hypertrophy" is like citing a 1993 study on one narrow population to justify a prescription for general-population clients three decades later. The citation is real. What it actually shows is much smaller.
Then came the Schoenfeld 2015 meta-analysis on time-under-tension, which reset the conversation. Schoenfeld and colleagues pulled together the available evidence on rep durations and muscle adaptations, and the finding was uncomfortable for the TUT framework: when volume and effort are matched, fast and slow tempos produce equivalent hypertrophy outcomes. The Mentzer/Hatfield-era hypothesis didn't survive controlled evidence. Schoenfeld never said "tempo never matters" (that's a misreading). What he said was that cadence isn't the differentiator the TUT framework predicted, once you control for the variables that actually drive hypertrophy.
So why does the tempo column persist in 2026, eleven years after the 2015 reset?
Three reasons.
First: template inheritance. Most online coaches build their first program templates from somewhere — a mentor's spreadsheets, a template store, an open-source PPL on Reddit. Those templates have tempo columns because they were built when tempo prescription was the default. Inheriting the convention isn't malpractice. It's how the industry moves. But inheriting it without auditing leaves a defensible-prescription gap that shows up the moment a client asks you to defend it.
Second: the "looks rigorous" signal. A program template with a tempo column looks more thoughtful than one without. The visual density of the spreadsheet signals thought to the client. That matters more than coaches admit when you're building your first ten clients and can't afford to look casual. The tempo column performs rigor whether or not the physiology supports the specific prescription. That's the theater part.
Third: the "intensification technique" framing. A lot of trainers still teach tempo as one of several intensification techniques alongside drop sets, rest-pause, and partial reps. In an in-person session where the coach is watching the lift and giving real-time cues, that framing has more defense than it does on a remote roster. Even in person, the evidence for tempo as a generic hypertrophy intensifier is thin once you control for effort and volume.
That's why the tempo column persists despite the underlying evidence: a transmission pattern, not a trainer's fault. The fix is to audit each prescription against the four-context decision tree and remove what fails.
2. What the evidence actually says (and doesn't say) about tempo and hypertrophy
The current evidence on tempo and hypertrophy is more interesting than either "tempo matters" or "tempo doesn't matter." Both readings miss the literature.
The headline from Schoenfeld 2015: when volume and effort are matched, faster cadences (≤ 2s per rep total) and slower cadences (4–8s per rep total) produce equivalent hypertrophy outcomes in trained and untrained populations. Not a fringe finding. It's been replicated across multiple subsequent studies and forms the basis of the modern consensus on cadence prescription for general-population hypertrophy work.
The literature isn't uniform, though. Two studies are often cited as the steelman for "tempo matters," and they deserve fair treatment. They're not wrong. They're just narrower than their template implementation assumes.
Mohamad et al. 2012 compared slow versus traditional tempo across hypertrophy training and found that the slow group produced different volume-load outcomes. The trials weren't effort-matched the way modern protocols control: the slow group performed fewer total reps at the same intensity. So the comparison was "different volume, different tempo," not "same volume, different tempo." The finding is real. The practical implication for a coach prescribing across 30 clients is narrower: if you're not effort-matching the protocol, the "slow tempo = different outcome" reading conflates cadence with volume, which the literature has separated for over a decade.
Schuenke et al. 2012 compared fast versus slow concentric tempos and found that type-II fiber recruitment responded differently to fast concentric movement. That has practical implications for power-and-strength athletes and narrower ones for general-population hypertrophy clients on conventional programming. The fast-concentric finding is real. The extrapolation that every hypertrophy client should be coached on fast concentric isn't what the data supports.
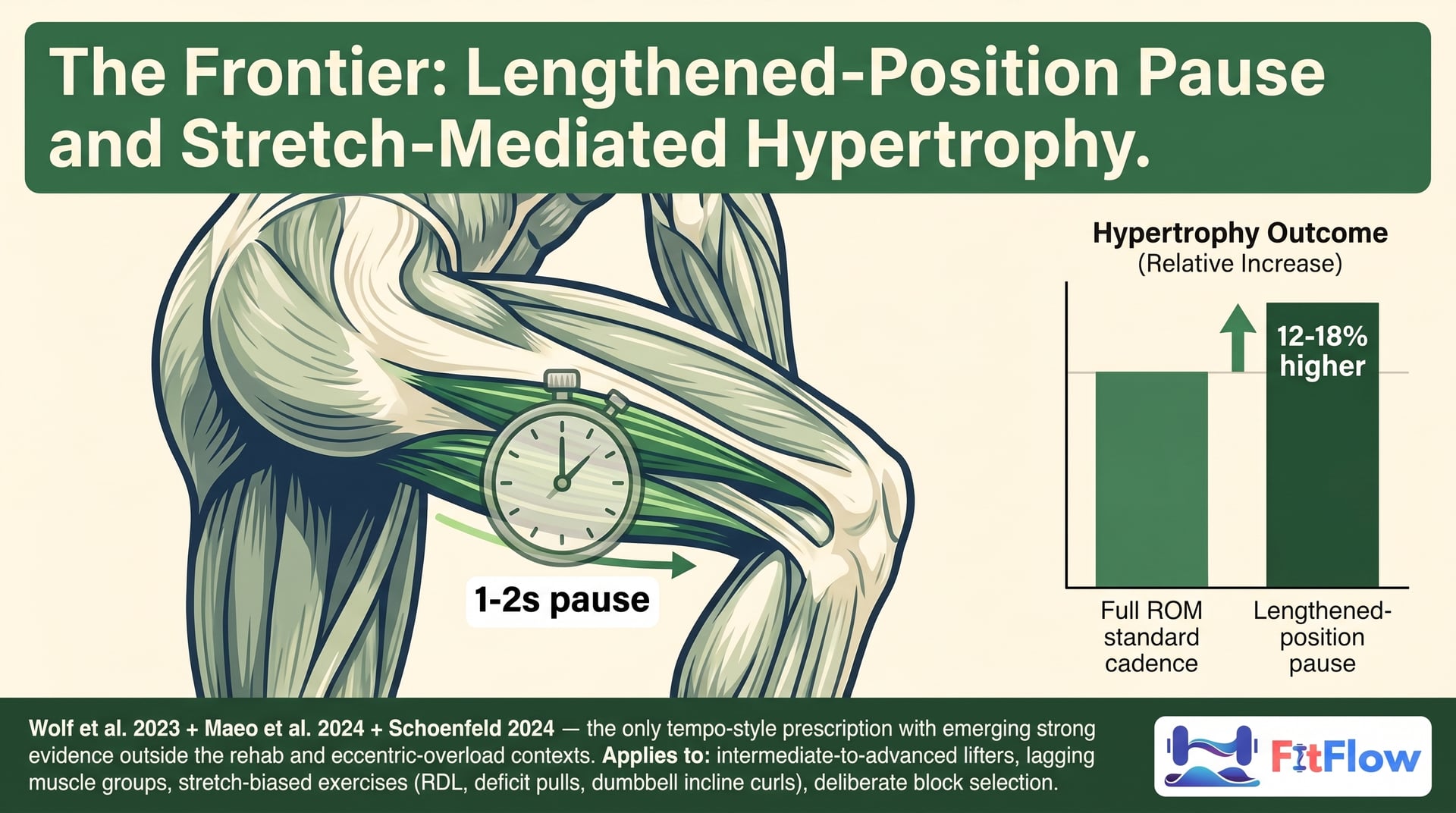
The 2024 update, captured in Schoenfeld's 2024 ROM/tempo synthesis, folds in the most recent lengthened-position hypertrophy literature (Wolf et al. 2023, Maeo et al. 2024) and shifts the conversation. The frame that emerged: cadence is downstream of effort and volume for general hypertrophy work, but the 1–2 second pause at the stretched position of stretch-biased exercises is the tempo-adjacent intervention with the strongest emerging hypertrophy signal. It's the only context where tempo-style prescription has growing evidence support outside the rehab and eccentric-overload domains. I treat that as Context #4 below.
Takeaway: tempo isn't a primary variable for hypertrophy programming. Effort (RPE/RIR) and volume (sets × reps × load) are primary. Range of motion is a strong secondary. Cadence sits downstream. That puts tempo on the bottom half of the leverage hierarchy described in the 80/20 of training results, which is the parent framing for this analysis. Tempo lives in the low-leverage segment, except in the four contexts below, where it crosses back into the leverage zone for specific, defined reasons.
The four contexts where tempo prescription is evidence-supported get their own sections next. The decision tree (Section 7) operationalizes the logic. The rest of this article gives you the prescriptions, the entry criteria, and the audit drill to clean up your roster.
3. Context #1: eccentric-overload protocols for advanced lifters
The first defensible context is eccentric-overload programming for advanced lifters in a specific macrocycle block.
The protocol is simple: prescribe a 4–6 second controlled eccentric (lowering) phase. The concentric phase can be explosive or self-selected; the eccentric is where the overload lives. Exercise selection should favor movements where the eccentric can be loaded heavily without joint-stress consequences — leg press, machine row, machine chest press, dumbbell variations.
The evidence base is strong but population-specific. Roig et al. 2009 published the original eccentric-vs-concentric meta-analysis, which established that eccentric training produces strength and hypertrophy effects with patterns distinct from concentric training. Douglas et al. 2017 extended that to supramaximal eccentric protocols (loads above the concentric 1RM, lowered controlled) and found specific strength-and-hypertrophy advantages in advanced lifters. That qualifier matters.
Roig 2009 and Douglas 2017 do not say every general-population hypertrophy client should be prescribed a 4-second eccentric on their bench press. They say that in advanced lifters with 2+ years of consistent training who have plateaued on conventional progression, eccentric-overload programming is a defensible block-cycle intervention for breaking through plateaus and continuing adaptation.
The decision criteria for Context #1 tempo:
Training age: 2+ years of consistent resistance training
Plateau marker: documented stagnation on conventional progression for 8+ weeks
Macrocycle position: a specific block (4–8 weeks) within the macrocycle dedicated to eccentric-overload work, not a permanent prescription
Exercise selection: movements that tolerate heavy eccentric loading without joint stress
Effort calibration: use eccentric-specific RPE; the eccentric phase should be hard but controllable through the full range
If any criterion fails, the eccentric-overload prescription isn't defensible. A novice prescribed 4-second eccentrics in their first program isn't in Context #1; they're in template-theater territory. A general-population intermediate client without a documented plateau, prescribed eccentric overloads on every set of every program, isn't in Context #1 either. The specificity matters.
The program-note template for Context #1 (full version in the Tempo Decision Guide) reads: "Block 3 eccentric-overload protocol. 4-second descent, self-selected concentric. Goal: continue overload progression after stalled volume progression in Block 2. Duration: 6 weeks. Transition back to self-selected cadence at start of Block 4."
That's what defensible Context #1 prescription looks like: tied to a specific client, a specific block, a specific objective, with a named transition out. A tempo column copy-pasted across every program in your roster doesn't qualify. This is a surgical intervention with documented entry and exit criteria. It also picks up the load-progression decision tree described in the progressive overload framework, where eccentric overload is named as one of the six load-progression dimensions. This article resolves that pointer with the specific cadence-prescription protocol.
4. Context #2: tendon-loading rehab and return-from-injury
Scope-of-practice note: this section addresses tempo prescription within tendon-loading rehab protocols. Tendon-loading prescription is part of an integrated rehab plan, not a substitute for clinical assessment. Refer clients with new, worsening, or unresolved tendon-mediated pain to a qualified physiotherapist for diagnosis before prescribing tempo work as a therapeutic loading strategy. The protocol described here is for use after diagnosis, within scope-of-practice, and under physiotherapist oversight where appropriate.
The second defensible context — and where the evidence is among the strongest in this article — is tendon-loading rehab for clients with diagnosed tendinopathy or in return-from-injury phases.
The protocol comes from two foundational citations. Cook & Purdam 2009 established the modern tendon-loading hierarchy: isometric loading → heavy slow resistance → energy-storage loading → plyometric/sport-specific. The heavy slow resistance phase is where tempo prescription becomes a primary protocol element rather than a programming flourish. Beyer et al. 2015 compared eccentric loading to heavy slow resistance training for patellar and Achilles tendinopathy and found that the heavy slow resistance protocol — 3-second descent + 3-second ascent on knee extensions and similar tendon-loading exercises — produced superior tendon adaptation outcomes.
The protocol for Context #2:
Pace: 3–6 second descent + 3–6 second ascent on tendon-loading exercises
Load: heavy enough to produce a hard 6–15 rep set; load progresses as symptoms permit
Exercises: tendon-specific selections (single-leg knee extensions for patellar; calf raises and isometric holds for Achilles; supraspinatus protocols for shoulder)
Frequency: 2–4 sessions per week, typically integrated with broader programming
Progression: track tendon-specific pain response (24-hour rule: pain that resolves within 24 hours is acceptable; pain that persists longer indicates over-loading)
This is the only context in this article where slow tempo is the primary protocol element rather than an optional intensification. The slow cadence is doing therapeutic work: it extends the load-duration to allow tendon-specific collagen synthesis to occur under sub-peak stress. Fast cadence doesn't provide that stimulus. Self-selected cadence in this population tends to drift too inconsistent for the therapeutic effect to register.
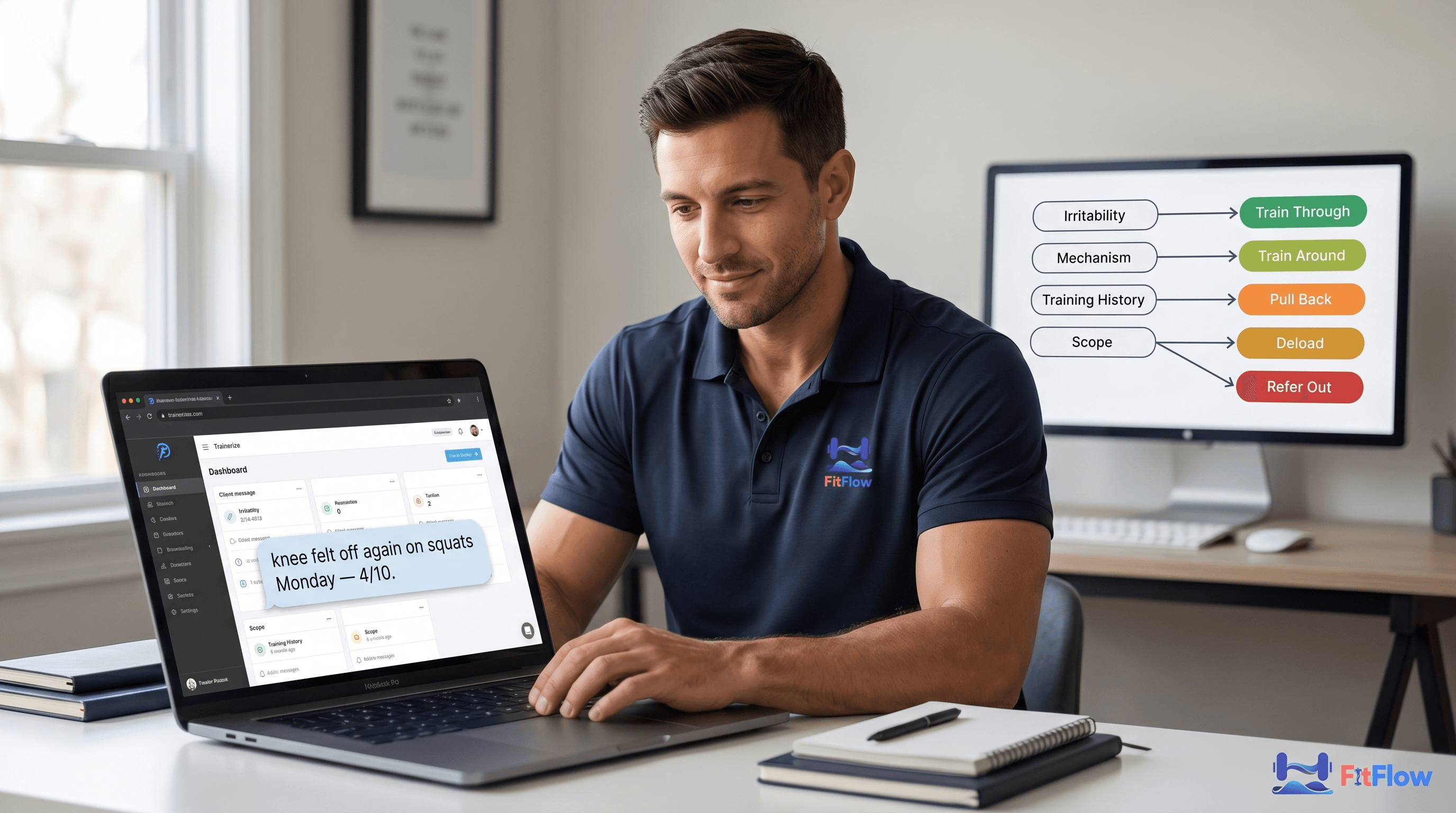
Context #2 cross-links directly to the chronic-pain decision tree, the parent decision tree for any pain-modification programming choice, which names slow eccentrics for tendinopathy as one of nine modifiable variables in its modifiable-variables menu. Read together: the chronic-pain decision tree tells you whether to train through, train around, or pull back; the tempo decision tree (this article) tells you which cadence protocol to prescribe inside the train-around branch when the pain-mechanism is tendinopathy.
The decision criteria for Context #2:
Diagnosis or strong indicator: tendinopathy diagnosis from physiotherapist OR clear mechanical-irritation presentation pointing to tendon-mediated symptoms (localized pain, load-tolerance dependence, gradual onset)
Phase: mid-to-late rehab or return-from-injury, NOT acute injury phase
Scope-of-practice: if diagnosis is unclear, refer; if symptoms worsen, refer; if the client has structural pathology requiring imaging or clinical intervention, refer
Integration: this is part of an integrated rehab plan, not a standalone prescription
Program-note template for Context #2 (full template in the Tempo Decision Guide): "Tendon-loading protocol. 3-second descent + 3-second ascent on knee extensions and split squats. Block duration tracks rehab phase (6–12 weeks typical). 24-hour pain rule: if pain persists beyond 24 hours, reduce load or contact me. Working under [physiotherapist name]'s oversight."
The scope-of-practice qualifier isn't bureaucratic boilerplate — it's the line that separates defensible Context #2 prescription from over-reach. The trainer is prescribing a loading strategy inside a rehab plan, not diagnosing or treating the underlying pathology.
Scope-of-practice reiteration: tendon-loading protocols described in this section assume a diagnosed condition under appropriate clinical oversight. For undiagnosed or worsening tendon-mediated pain, refer to a qualified physiotherapist before prescribing tempo work as a therapeutic strategy.
Get the Tendon-Rehab program-note template (full Tempo Decision Guide, free)
5. Context #3: technique / motor-learning phase for novices
The third defensible context is technique-stabilization tempo prescription for novice clients in their first 4–12 weeks.
The protocol is brief and time-limited: prescribe a controlled cadence (2–3 second descent, brief pause at the bottom, controlled ascent) on the compound lifts where the novice is still building motor patterns. This is a teaching tool, not a hypertrophy stimulus. The slow cadence creates cognitive bandwidth for the novice to attend to proprioceptive feedback, bar-path stability, and range-of-motion consistency. Once the motor pattern stabilizes (typically within 4–8 weeks of consistent practice), the prescription is withdrawn and the client moves to self-selected cadence with periodic technique-QA.
The evidence base for Context #3 comes from the motor-learning literature, particularly the specificity-of-practice principle articulated by Schmidt & Lee and the broader cognitive-motor literature on skill acquisition. Slow practice creates cognitive bandwidth; bandwidth allows attention to feedback; attention to feedback drives skill consolidation. That chain is well-established outside the hypertrophy literature and applies to resistance training as a special case.
The decision criteria for prescribing Context #3 tempo:
Training age: less than 6 months of consistent resistance training
Observable indicator: bar-path instability OR range-of-motion inconsistency OR rep-to-rep variation that suggests the motor pattern is not yet stable
Time-bounded: maximum 8–12 weeks; prescription is withdrawn once the motor pattern stabilizes
Exercise selection: compound lifts where the motor pattern is being learned (squat, deadlift, overhead press, bench press); not isolation work where motor learning is less load-bearing
Transition plan: a specific transition checkpoint at 4–8 weeks where the prescription is re-evaluated and either continued, modified, or withdrawn
The critical qualifier for Context #3 is temporary. The novice still being coached on a 3-1-1-0 tempo at month nine isn't in Context #3 anymore. They're in template-theater territory. The transition out of Context #3 is as important as the entry into it.
Operationally, Context #3 is the cleanest case for tempo prescription on a 20–50 client roster. You have a small number of clients in their first 12 weeks at any given time — typically 10–20% of an established roster. Inside that subset, the technique-tempo prescription is defensible and bounded. Outside it, it isn't.
A program-note template for Context #3: "Technique stabilization phase. 2-second descent, 1-second pause at bottom, controlled ascent on squat / deadlift / press. Goal: motor-pattern stabilization. Transition to self-selected cadence at Week 8 check-in pending technique audit." That's the template the Tempo Decision Guide expands into full copy.
Context #3 also resolves a pointer from the variable-rotation anti-pattern, which warns against rotating exercises to manufacture novelty without programmatic justification. The technique-tempo prescription is a defensible variable-pattern intervention because it has a specific learning objective and a transition plan. "Rotating tempo every block to add variety" is the anti-pattern that piece warns against.
6. Context #4: stretch-mediated hypertrophy / lengthened-partial protocols
The fourth context — and the one with the most interesting emerging evidence — is lengthened-position tempo prescription inside stretch-mediated hypertrophy protocols.
This is where the 2023–2024 literature has moved the conversation in ways the 2015 Schoenfeld synthesis couldn't anticipate. Wolf et al. 2023 published a meta-analysis on lengthened partials (partial-range-of-motion training emphasizing the stretched position) and found a consistent hypertrophy advantage over full-range training in stretch-biased exercises. Maeo et al. 2024 extended that with controlled comparisons of partial versus full ROM hypertrophy outcomes. Schoenfeld 2024 folded the findings into the updated range-of-motion synthesis.
The tempo-specific implication: a 1–2 second pause at the lengthened (stretched) position in stretch-biased exercises produces measurable hypertrophy effects that other tempo prescriptions do not. It's the only context where a tempo-style prescription has emerging strong evidence outside the rehab and eccentric-overload domains.
The protocol:
Pace: 1–2 second pause at the lengthened (stretched) position; concentric and eccentric self-selected
Exercise selection: stretch-biased exercises where the stretched position carries the hypertrophy stimulus
Hamstrings: Romanian deadlift, stiff-leg deadlift
Lats: deficit pull-ups, dumbbell pullovers
Long-head biceps: incline dumbbell curls
Long-head triceps: overhead extension variations
Quads: deep squat variations, sissy squats
Population: intermediate-to-advanced lifters with at least 12 months of consistent training
Block selection: used in specific blocks targeting lagging muscle groups, not a universal prescription
The decision criteria for Context #4:
Training age: 12+ months consistent resistance training (intermediate or above)
Target identification: a specific lagging muscle group has been identified and the block is being structured around it
Exercise type: the selected exercise places the hypertrophy stimulus at the lengthened position (this is exercise-specific; not every exercise has this property)
Deliberate block selection: this is a block-specific intervention, not a universal cadence prescription
The mechanism merits brief comment because it's where the evidence frontier is moving. Stretch-mediated hypertrophy appears to interact with the muscle's mechanical loading at long muscle lengths in ways the lengthened-position pause amplifies. The 1–2 second pause provides time for the tissue to experience load at the position where the stretch-mediated stimulus operates. That's distinct from the older "slow concentric for hypertrophy" framing — the cadence here is being used to access a specific mechanical-loading position, not as a generic stimulus. The distinction matters for prescription.
A program-note template for Context #4: "Block 4 lengthened-position protocol. 1-second pause at stretched position on RDL (hamstrings) and incline DB curl (biceps long head). Targeting lagging muscle groups identified in Week 1 audit. Block duration: 6 weeks. Transition back to self-selected cadence at Block 5." Specific, bounded, with a transition.
This context will probably expand as the literature matures. The ACSM 2026 Position Stand (expected Q3 2026) will likely codify lengthened-position evidence into mainstream guidance, which will be a refresh trigger for this article and the broader programming-design content. Until then, Context #4 is the frontier-but-defensible tempo prescription for the operational coach who wants to deploy emerging-evidence interventions surgically rather than wholesale.
7. The 4-context decision tree (operational asset)
Time to operationalize the four contexts into a single decision tree you can audit your roster against this week.
The tree runs as a sequential check. Default branch: no tempo prescription, self-selected cadence with controlled execution. The four contexts are exceptions, each with specific entry criteria. If a client × exercise pair clears one of the four entry checks, prescribe the corresponding tempo. If none clear, drop the tempo column.
The tempo prescription decision tree:
START — For each client × exercise pair on the roster:
Step 1: Is this an eccentric-overload-block-programmed prescription?
── Training age 2+ years?
── Documented plateau on conventional progression (8+ weeks)?
── Specific 4–8 week block dedicated to eccentric overload?
── Exercise tolerates heavy eccentric loading?
YES to all → PRESCRIBE Context #1 (4–6s eccentric descent, self-selected concentric)
ANY NO → Go to Step 2
Step 2: Is this a tendon-loading rehab prescription?
── Tendinopathy diagnosis OR clear tendon-mediated symptoms?
── Mid-to-late rehab phase (not acute)?
── Scope-of-practice cleared (under physiotherapist oversight where appropriate)?
YES to all → PRESCRIBE Context #2 (3–6s descent + 3–6s ascent, heavy slow resistance)
ANY NO → Go to Step 3
Step 3: Is this a technique-stabilization phase prescription?
── Training age less than 6 months?
── Observable technique breakdown OR motor-pattern instability?
── Compound lift where motor learning is load-bearing?
── Transition plan documented for 4–8 weeks out?
YES to all → PRESCRIBE Context #3 (2–3s descent, brief pause, controlled ascent)
ANY NO → Go to Step 4
Step 4: Is this a lengthened-partial-block prescription?
── Training age 12+ months (intermediate or above)?
── Specific lagging muscle group identified?
── Stretch-biased exercise where lengthened position carries the stimulus?
── Deliberate block selection (not universal cadence prescription)?
YES to all → PRESCRIBE Context #4 (1–2s pause at lengthened position)
ANY NO → DROP TEMPO COLUMN, prescribe self-selected cadence with controlled execution
END

The visual version of this tree appears as an infographic mid-article and inside the Tempo Decision Guide. The text version above is the operational one you can paste into your roster-audit workflow.
A few critical notes.
The default branch is "no tempo prescription." If a client × exercise pair doesn't clear one of the four entry checks, drop the tempo column. That's evidence-grounded programming, not casual programming. Self-selected cadence with controlled execution is the evidence-supported default for general-population hypertrophy work in the 5–30 rep range.
Multiple contexts can apply. A client returning from tendinopathy who's just transitioned out of rehab and into a hypertrophy-focused block could have Context #2 prescriptions on tendon-loading exercises and Context #4 prescriptions on lengthened-partial exercises in the same program. The decision tree runs per client × exercise, not per client. That's the operational point that makes the tree scale to 30+ client rosters: you're not deciding "tempo or not" for the whole client; you're deciding per exercise.
It composes with the elite-coaches decision-triage framework, which describes the meta-decision approach for any coaching call. The tempo decision tree is the tempo-domain instantiation of that meta-pattern. Together: the meta-pattern tells you HOW to decide; the tempo decision tree tells you WHAT to decide for tempo specifically.
It also composes with the RPE vs RIR decision tree, the sister decision tree for effort prescription. The two trees run independently per client and per exercise. Effort prescription is the higher-leverage decision; tempo prescription is downstream. I address the relationship between the two in Section 9 below.
8. Roster segmentation: who gets tempo this block, who doesn't
Once you have the decision tree, the next operational question: across your full 20–50 client roster, who actually gets tempo prescriptions this block, and who doesn't?
The roster-segmentation table (full version in the Tempo Decision Guide) cuts your roster along three dimensions: client archetype (novice / intermediate / advanced), training goal (hypertrophy-focused / strength-focused / general-fitness / rehab-modified), and injury history (none / past-resolved / current-modified). The intersection tells you roughly which clients are candidates for which of the four contexts.
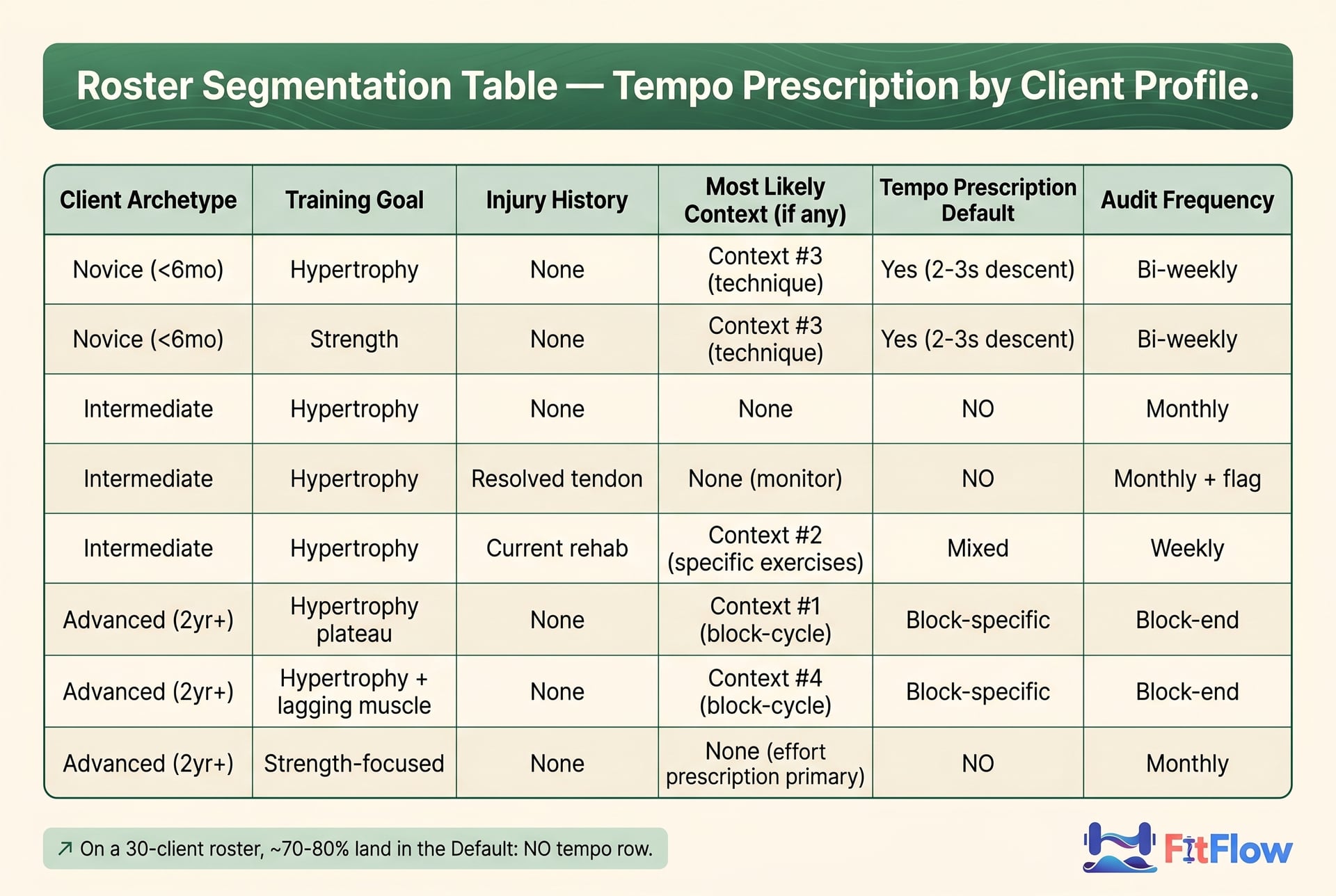
If you run the decision tree across a typical 30-client online roster, the distribution typically lands somewhere like this:
No tempo prescription (self-selected cadence with controlled execution): ~21–24 clients
Context #1 (eccentric overload): ~1–3 clients in any given block, typically only when an advanced client has hit a documented plateau and you're cycling them through an eccentric-overload block
Context #2 (tendon rehab): ~1–4 clients on any given week, depending on injury prevalence in the roster
Context #3 (novice technique): ~3–6 clients at any time, the cohort in their first 4–12 weeks
Context #4 (lengthened-partial): ~1–4 clients in any given block, those who have identified lagging muscle groups and are running a stretch-biased block
The numbers shift with your client mix. A roster heavily weighted toward advanced lifters will see more Context #1 and #4 activity. High beginner intake means more Context #3. Active rehab work means more Context #2.
The total tempo-prescription count across the roster stays small. Roughly 20–30% of clients have a defensible tempo prescription on any given block, and even inside that subset, the prescription usually applies to a few of their exercises rather than every exercise on every program. The tempo column is sparse, not universal.
That's the operational reframe. The tempo column on your client's program isn't a default — it's a selectively-applied intervention, prescribed per client per exercise after the decision tree clears one of four entry checks. The roster-segmentation table is the operational artifact that makes this prescribable at scale. Without it, you're either (a) prescribing tempo universally and accumulating tempo-theater entries, or (b) dropping tempo universally and missing the four contexts where it does work.
The monthly audit cadence (described in Section 11) keeps the roster-segmentation table accurate as clients transition between contexts. A novice in Week 6 of Context #3 transitions out of tempo prescription at Week 8–12 as their motor pattern stabilizes. A client finishing a Context #1 eccentric-overload block transitions back to self-selected cadence for the next block. A tendinopathy client clearing Context #2 transitions out of the rehab-tempo prescription as symptoms resolve. The audit is what keeps those transitions clean rather than letting Context-anchored prescriptions decay into template-theater.
Get the full Roster Segmentation Table (free Tempo Decision Guide)
The reframe has a quiet retention benefit worth naming. Tempo compliance is a measurable retention leak on remote rosters: clients prescribed tempos they don't understand (or don't see the point of) develop subtle disengagement signals that compound over the month-3 attrition window. Dropping the tempo prescriptions that don't clear the decision tree removes a hidden compliance friction.
It also connects to the operations playbook for online coaches managing 30+ client rosters, which names roster-template QA as one of the seven operational systems. The tempo audit described here is the tempo-domain instantiation of the template-QA system in that playbook.
9. Tempo vs. effort (RPE/RIR): which variable should you prescribe?
If you can only add one variable to load and reps on your client's program, prescribe effort (RPE or RIR), not tempo. That's the practical resolution of the tempo-vs-effort question.
Effort is the load-bearing variable for hypertrophy. The Schoenfeld 2015 meta-analysis and its successors establish this consistently: hypertrophy responds to effort × volume more than to any other prescribed variable. Cadence is downstream. Prescribe tempo without controlling effort and you've added variability without controlling the variable that actually drives the adaptation.
Tempo and effort interact in confusing ways, which is why this matters. Prescribe a 4-second eccentric on a set of squats and the client performs 10 reps, and their per-rep effort is different than if they had performed 10 reps with self-selected cadence. The slow cadence has changed the effort signature, but as a side-effect, not as an intentional effort prescription. If you wanted to prescribe effort, you should have prescribed effort directly: "Squat for 10 reps at RPE 8" tells the client what to do. "Squat for 10 reps with 4-second descent" leaves the effort uncontrolled and adds a cadence variable that may or may not be doing useful work.
The cleanest operational decision: prescribe effort first, prescribe tempo only when the four-context decision tree clears. When the four contexts have specific reasons to prescribe tempo as well, tempo gets added on top of effort. When the tree doesn't clear, tempo comes off entirely and effort prescription continues. The cadence becomes whatever the client self-selects to hit the prescribed effort target.
This relationship sits at the intersection of RPE vs RIR for online coaching and this article. The RPE vs RIR piece is the deep treatment of effort prescription: scalability across 20–50 client rosters, novice-vs-advanced calibration, platform-vocabulary alignment. This article is the tempo prescription deep treatment. The relationship: effort > tempo as a prescription priority in 80% of decisions, with tempo entering only when the four-context decision tree clears.
A two-line program-note pattern that captures the relationship: "Effort target: RPE 8 (2 reps in reserve). Cadence: self-selected, controlled execution." That's the default. For Context #1: "Effort target: RPE 8. Cadence: 4-second eccentric, self-selected concentric." For Context #4: "Effort target: RPE 8. Cadence: 1-second pause at lengthened position." The effort prescription is the constant; cadence enters as a context-specific overlay.
That's the practical resolution. Most online coaches over-prescribe tempo and under-prescribe effort. Inverting the priority — and using the four-context decision tree to determine when tempo enters at all — is the operational shift that cleans up the roster and concentrates prescription on the variables that actually move hypertrophy outcomes.
10. Case study: two online clients, two tempo decisions
To make the decision tree concrete, here are two clients from a typical online roster with paired tempo decisions. The contrast shows how the tree resolves different cases. Both are composites — drawn from common patterns rather than any single client.
Client A: Marcus
Profile: 32 years old, 3 years consistent training, intermediate hypertrophy goal, no injury history
Current programming: 4-day upper/lower split, 5–12 rep range, conventional progression
Status: steady progress on volume-load progression over the past 6 weeks; no plateau signal
Decision tree run:
Step 1 (Context #1, eccentric overload): training age clears, but NO documented plateau. Step 1 fails.
Step 2 (Context #2, tendon rehab): no tendinopathy diagnosis or symptoms. Step 2 fails.
Step 3 (Context #3, novice technique): training age > 6 months. Step 3 fails.
Step 4 (Context #4, lengthened-partial): no specific lagging muscle group identified and no stretch-biased block selected. Step 4 fails.
Default branch reached: NO tempo prescription. Self-selected cadence with controlled execution.
Program note (post-decision): "Effort target: RPE 8 on top sets; RPE 7 on back-off sets. Cadence: self-selected, controlled execution. No tempo prescription this block."
Audit reasoning documented: "Marcus is making steady progress on conventional load + effort prescription. No context in the decision tree clears. Tempo column removed from the program template effective this block."
Marcus is in the 70–80% of the roster where tempo prescription is theater. The decision tree formalizes that. Removing the tempo column doesn't depress his hypertrophy outcomes — the literature says it shouldn't, and the next 12 weeks of programming will confirm or refute on his individual data.
Client B: Sarah
Profile: 36 years old, 5 years consistent training, advanced hypertrophy goal, returning from diagnosed right-side patellar tendinopathy (under physiotherapist oversight; cleared for graduated loading)
Current programming: 4-day upper/lower split, currently in Week 4 of rehab-modified return-to-training
Status: tendinopathy symptoms resolving on physiotherapist-prescribed heavy slow resistance protocol; cleared for graduated programming integration
Decision tree run (per exercise):
For single-leg knee extension (tendon-loading exercise): Step 2 (Context #2, tendon rehab) clears. Prescribe 3-second descent + 3-second ascent.
For dumbbell incline curl (Sarah has identified biceps long-head as a lagging muscle group; she's running a stretch-biased block on upper-body exercises): Step 4 (Context #4, lengthened-partial) clears. Prescribe 1-second pause at lengthened position.
For squat (compound lift, not tendon-targeted): Steps 1–4 all fail. Default branch: NO tempo prescription.
For bench press (compound lift, not tendon-targeted, not in lengthened-partial block): Steps 1–4 all fail. Default branch: NO tempo prescription.
Program note (post-decision): "Effort target: RPE 7–8. Cadence: 3-second descent + 3-second ascent on knee extensions and split squats (tendon-loading protocol). 1-second pause at lengthened position on incline DB curls (lengthened-partial block, targeting biceps long head). Self-selected cadence on all other exercises. Working under [physiotherapist name]'s oversight on the tendinopathy protocol. 24-hour pain rule applies: contact me if pain persists past 24 hours."
Cross-link to the chronic-pain decision tree: Sarah's case bridges to that tree. The prior step in her programming chain was the pain-modification decision (train through, train around, or pull back), which the chronic-pain decision tree handles. The tempo decision tree (this article) handles the cadence-prescription decision once the chronic-pain decision tree has resolved.
Sarah is in the 20–30% of the roster where tempo prescription is defensible — and even inside Sarah's program, tempo applies only to specific exercises, not to her entire program. The decision tree running per exercise (not per client) is what keeps this operationally clean.
The contrast between Marcus and Sarah shows the operational point: tempo prescription isn't a binary client-level decision. It's a per-exercise decision driven by the four-context decision tree. Most client × exercise pairs fail all four entry checks and land at the default branch (no tempo prescription, self-selected cadence). A small subset clears one of the four checks and receives a specific, defensible prescription.
11. How to audit your existing roster's tempo prescriptions this week
The audit drill is a 5-step process you can run on your full roster in roughly 2–4 hours of focused work. Full version with worksheets in the Tempo Decision Guide.
Step 1: pull all current program templates (15–30 minutes)
Open every active client's program in your coaching platform. Export or screenshot the current week's prescription for each. The artifact you're auditing is the spreadsheet (or app prescription) as it exists today, not what you wish it said.
Step 2: count which programs have tempo columns (15 minutes)
For each program, note whether the tempo column is populated (any tempo notation on any exercise). Tally the count. Most online coaches doing this audit for the first time find ~70–90% of programs have populated tempo columns. That's the baseline.
Step 3: for each program with tempo, classify against the 4 contexts (60–120 minutes)
For each program with populated tempo columns, run the decision tree per exercise. Document the result in a single line per client:
"Client name — Exercise — Tempo prescribed — Context check result: Context #_/None — Action: Keep / Modify / Drop"
This is the load-bearing step. Most of the audit time goes here. Be honest in the classification: if you can't defend the prescription against one of the four entry checks, the action is Drop, not Keep.
Step 4: drop tempo from any program that fails the 4-context test (30–60 minutes)
For every "Drop" action from Step 3, edit the program template to remove the tempo column or set the tempo to "self-selected, controlled execution" for that exercise. Save the edited programs. The roster's tempo column is now sparse, populated only on the exercises and clients where the decision tree cleared.
Step 5: update program notes to explain the change to the client (30–60 minutes)
For every client whose program changed in Step 4, send a brief message (or update the program note) explaining the change. A template that works:
"I've audited your program against the latest evidence on tempo prescription for hypertrophy. The slow tempos I had prescribed on [exercises] were inherited from a template convention; the evidence (Schoenfeld 2015 + 2024) shows that for your training goal, self-selected cadence with controlled execution produces equivalent results. The exercises where I'm keeping the tempo prescription [if any] are [list with rationale]. Effort prescription (RPE/RIR) continues as the primary cue. Let me know if you have questions."
Don't skip this step. Changing the client's program without explanation creates anxiety. A three-sentence evidence-backed explanation builds trust and trains the client to expect data-driven programming decisions from you.
Audit output
After the 5-step audit, your roster will typically show:
70–80% of clients have NO tempo prescriptions (tempo column removed or set to self-selected)
20–30% of clients have tempo prescriptions on a subset of their exercises (the contexts that cleared)
100% of remaining tempo prescriptions are documented with a specific Context (#1, #2, #3, or #4) and a transition plan
That's the operational state after the audit. The monthly cadence (re-running Step 3 for any new clients or clients whose status has changed) keeps the roster aligned with the decision tree as clients transition between contexts.
Run the audit on your roster this week. The free Tempo Decision Guide includes the 4-context decision tree, the 5-step audit drill, the program-note templates, the tempo-vs-effort map, the troubleshooting playbook, and the quick reference card. 9 operational assets. One download. Free. Get the Free Tempo Decision Guide.
Frequently Asked Questions
Comments