Why Your Clients Are Not Recovering
Your clients are already talking about their cortisol. They have watched the TikTok videos, absorbed the Huberman episodes, arrived at sessions with a vocabulary for stress physiology that did not exist two years ago. The cortisol spike meme has crossed from niche wellness discourse into the mainstream. Your clients understand, at least intuitively, that their bodies are stressed and their recovery is compromised.
Here is the problem: their understanding is mostly correct, and their trainer's diagnostic framework is mostly missing. Understanding why clients are not recovering requires looking far beyond the training program itself.
Every major 2026 fitness industry report — Trainerize, MyPTHub, Everfit, ACSM — now names recovery monitoring as a top-three professional skill for personal trainers. The industry has decided recovery is in scope. The question is whether trainers have the diagnostic tools to deliver.
Your clients do not need a better program. They need a recovery system. You are optimizing 5 hours of weekly training and systematically ignoring the 163 hours that actually determine whether those 5 hours produce results. If your clients are plateauing, losing motivation, or showing signs of chronic fatigue, the answer is probably not in the program. It is in the 163 hours you are not assessing.
Audit Your Client's Recovery Before the Next Plateau Hits. Get the Free Checklist.
This article is not a comprehensive recovery toolkit — for that, see our Evidence-Based Nutrition & Recovery Guide. This is a diagnostic guide. It identifies the 5 specific hidden barriers that trainers consistently fail to assess: the gaps between what you program and what your clients actually experience during the other 163 hours of their week.
Whether you manage 20 clients and need a systematic framework to audit recovery failure across your roster, or you are an evidence-based fitness enthusiast trying to understand why your own body is not responding to training — the diagnostic structure is the same.
The Overtraining Myth: Why the Wrong Diagnosis Is Costing Your Clients Results
The difference between overtraining and under-recovering is not semantic. It is the difference between a rare clinical condition and a common programming failure — and most trainers only know how to diagnose the first one.
Overtraining Syndrome (OTS) is a pathological state — persistent performance decrements that do not resolve with normal recovery, along with hormonal disruption, immune suppression, and psychological disturbance. OTS is real, serious, and rare. The PMC Practical Guide to Overtraining Syndrome established the clinical criteria most certifications teach.
The problem: OTS is virtually the only recovery failure framework most trainers learn. This creates a diagnostic blind spot. When a client presents with fatigue and declining performance, trainers either dismiss it because it does not meet OTS criteria, or overreact and prescribe complete rest when targeted programming adjustments would suffice.
What most trainers actually encounter is not OTS. It is a point on the overreaching continuum:
Functional overreaching: Short-term, performance-beneficial. Recovery takes days to weeks. This is a normal part of progressive training.
Non-functional overreaching: Recovery takes weeks to months. Performance deficits persist despite standard recovery. This is the danger zone — and it is where most "stuck" clients live.
Overtraining Syndrome: Rare, clinical, severe. Recovery takes months to years.
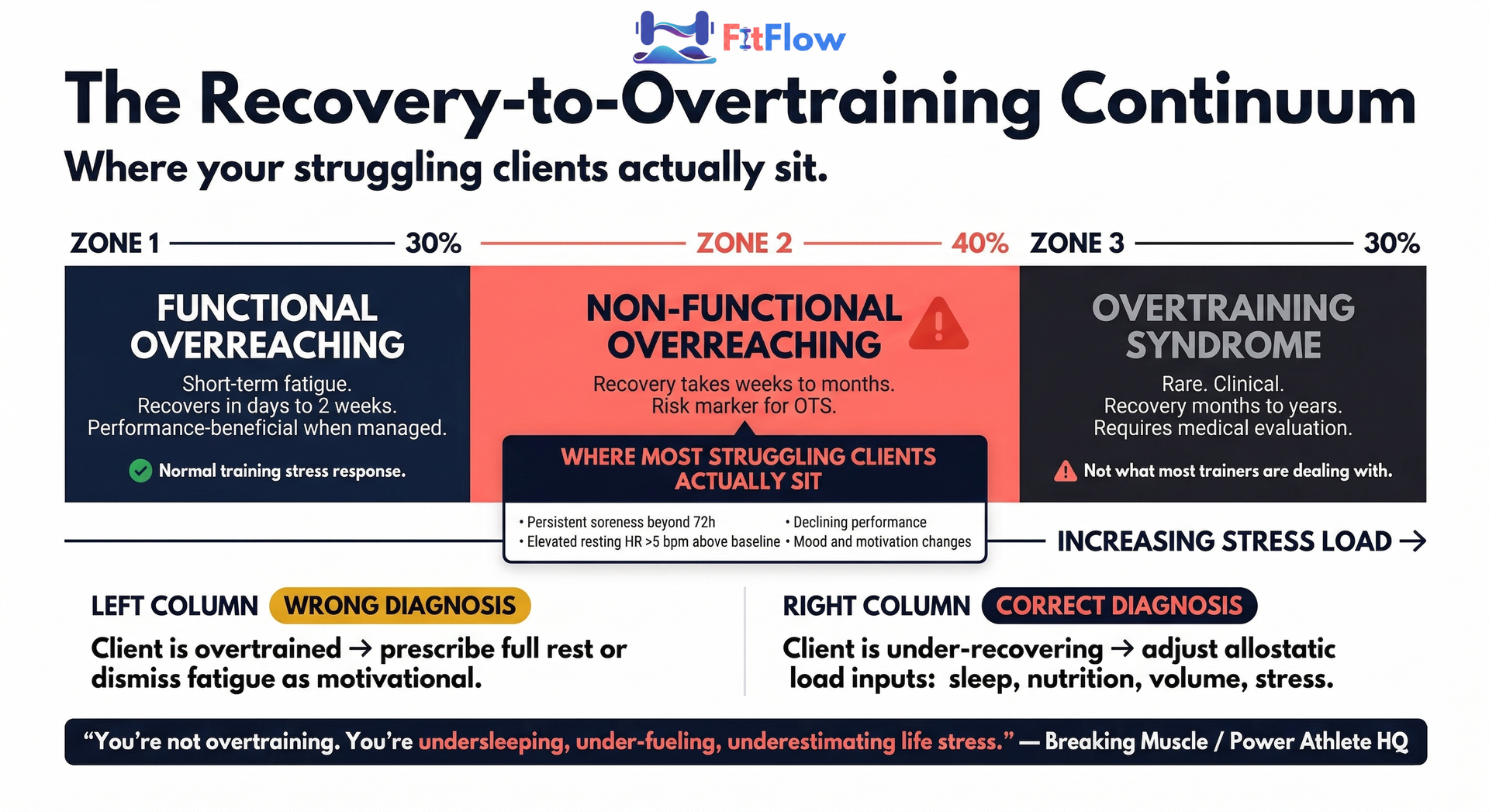
As Dr. Marco Neri articulated at the Summit of Strength 2026: "Overtraining is the accumulation of stress from training AND external factors — diet, sleep, psychological stress." The majority of clients whose performance is declining are not overtrained. They are under-recovering. Same symptoms. Different cause. Completely different fix.
The reframe that changes everything: you are not overtraining your clients. You are undersleeping them. You are under-fueling them. You are underestimating how much the rest of their life costs their body.
You control 5 hours of training per week. Your client controls 163 hours of everything else — sleep, nutrition, stress, hydration, movement, social demands. If you are not assessing the 163 hours, you are programming in the dark.
We have previously argued that the most important system gap is not in your programming — it is in your intake and assessment process. Recovery failure is one of five system breakdowns that scaling trainers must address. This article is the diagnostic layer for the most invisible of those breakdowns.
What the Research Calls It vs. What Trainers Actually See
Functional overreaching is the practitioner-relevant category. Here are the specific diagnostic markers that most trainers see in clients but misattribute to "motivational issues" or "just a bad week" — without connecting them to programming decisions:
Persistent muscle soreness beyond 72 hours: If a client reports DOMS lasting four or more days from sessions that used to produce 24-48 hour recovery, the recovery system is failing.
Declining performance despite adequate reported sleep and nutrition: Strength loss on lifts that were progressing two weeks ago — without a clear programming explanation — is an overreaching signal.
Elevated resting heart rate: A sustained increase of more than 5 beats per minute above baseline for three or more consecutive days indicates sympathetic nervous system dominance and insufficient recovery.
Mood and motivation shifts: Irritability, reduced training enthusiasm, and disrupted sleep patterns in a client who was previously engaged are not personality problems. They are physiological signals that the recovery system is overwhelmed.
If two or more are present simultaneously, the client is not having a bad week. They are in non-functional overreaching, and the program needs to respond.
Hidden Barrier 1: Sleep Is Not a Lifestyle Preference. It Is a Programming Variable.
Most trainers know sleep matters. Almost no trainer systematically asks about sleep architecture — not just how many hours, but sleep quality, timing consistency, and the factors that disrupt recovery phases within sleep — or adjusts programming based on what clients report. Sleep sits in the "things I tell clients to improve" category, not the "data I use to make programming decisions" category. That is the gap.
Here is what sleep deprivation actually costs:
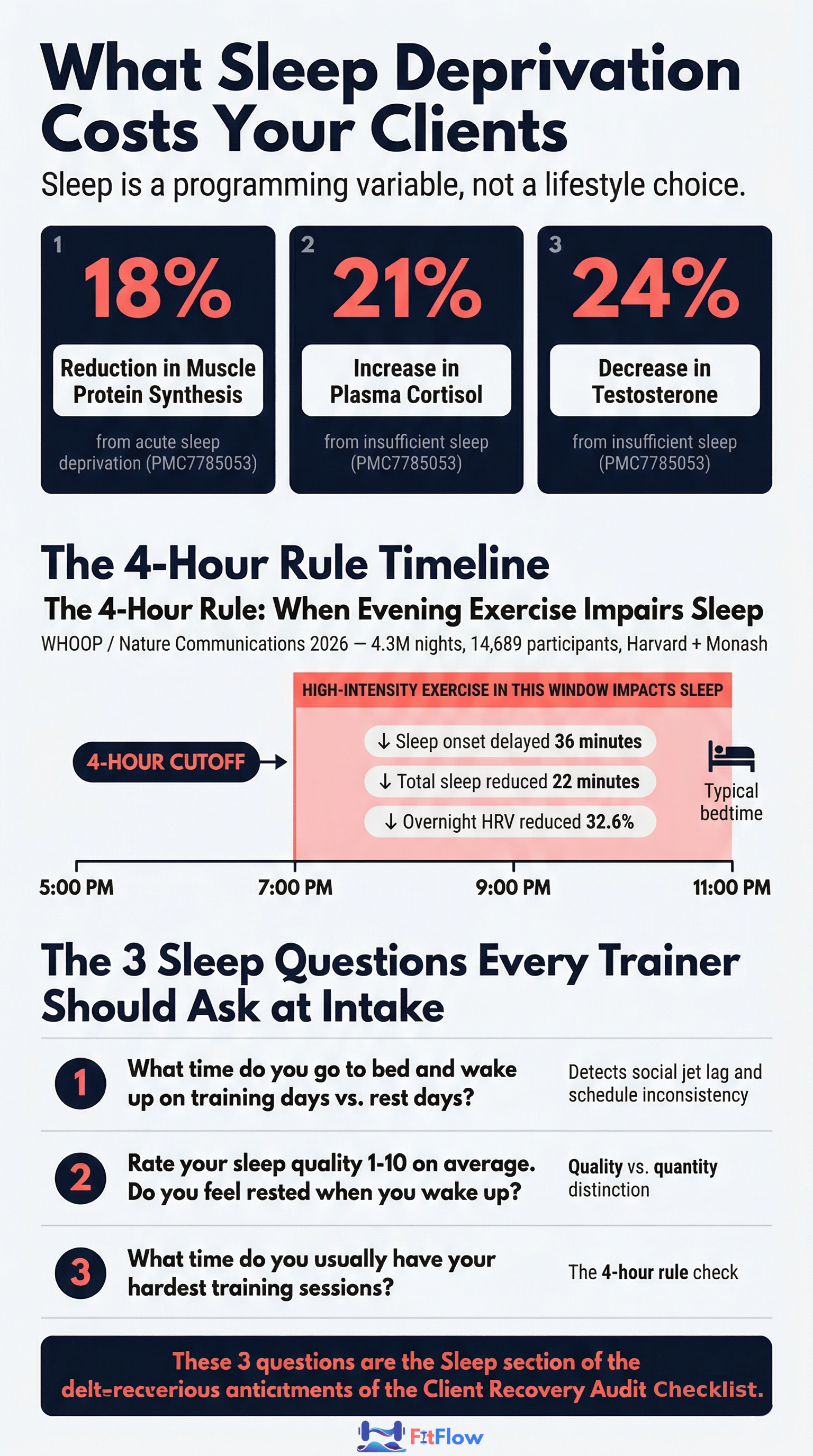
Acute sleep deprivation reduces muscle protein synthesis by 18%, increases plasma cortisol by 21%, and decreases testosterone by 24% (PMC7785053)
Disrupted slow-wave sleep (the N3 phase) suppresses growth hormone secretion during the critical post-training repair window
Elevated pro-inflammatory cytokines (IL-6, CRP) from chronic sleep restriction directly impair tissue repair and extend recovery timelines
Sleep fragmentation — waking multiple times per night — degrades recovery even when total sleep duration appears adequate
The most significant finding from 2026 comes from the landmark WHOOP/Nature Communications study — 4.3 million nights of sleep data from 14,689 participants, conducted by researchers at Harvard and Monash University. High-intensity exercise within 4 hours of bedtime delays sleep onset by 36 minutes, reduces total sleep by 22 minutes, and produces a 32.6% decrease in HRV. As Bryan Johnson noted when sharing the study: avoid high-intensity exercise close to bedtime if you value recovery.
If you are programming late-evening high-intensity sessions without asking what time clients go to bed, you may be systematically degrading their most powerful recovery mechanism.
A client sleeping 8 hours with fragmented sleep architecture recovers substantially worse than the same client sleeping 7 hours of consolidated, high-quality sleep. Duration is the metric people report. Architecture is the metric that determines recovery.
At the 2026 Milano Cortina Winter Olympics, Team USA's performance team deployed a dedicated sleep working group, identifying sleep as "a factor that can put athletes in an incredible competitive position." If Olympic coaches treat sleep as a formal programming input, it belongs in every trainer's intake process.
For the complete evidence-based sleep optimization protocol — including specific timing recommendations, environment modifications, and supplementation research — see our Evidence-Based Nutrition & Recovery Guide.
The 3 Sleep Questions Every Trainer Should Ask at Intake
These are not general wellness check-ins. They are diagnostic questions that feed directly into programming decisions:
"What time do you usually go to bed and wake up on training days vs. non-training days?" Identifies sleep consistency and social jet lag. A client who sleeps 11 PM-7 AM on training days but 1 AM-10 AM on weekends has a circadian disruption problem no supplement will fix.
"Do you feel rested when you wake up? Rate sleep quality 1-10." Distinguishes duration from quality. A client sleeping 8 hours but rating quality 4/10 has a sleep architecture problem, not a duration problem.
"What time do you schedule your hardest training sessions?" The 4-hour rule check. If a client trains at high intensity at 8 PM and sleeps at 10:30 PM, the WHOOP/Nature study shows a measurable recovery cost. The fix may be as simple as shifting the session earlier.
These 3 questions form the Sleep section of the Client Recovery Audit Checklist. They take 2 minutes to ask. They change how you program.
Hidden Barrier 2: Your Client's Life Is Doing More Reps Than You Are
Your clients are calling it "cortisol spiking." They are right, but only partially. Cortisol is one signal of a much larger physiological pattern called allostatic load — and your programming may be making it worse.
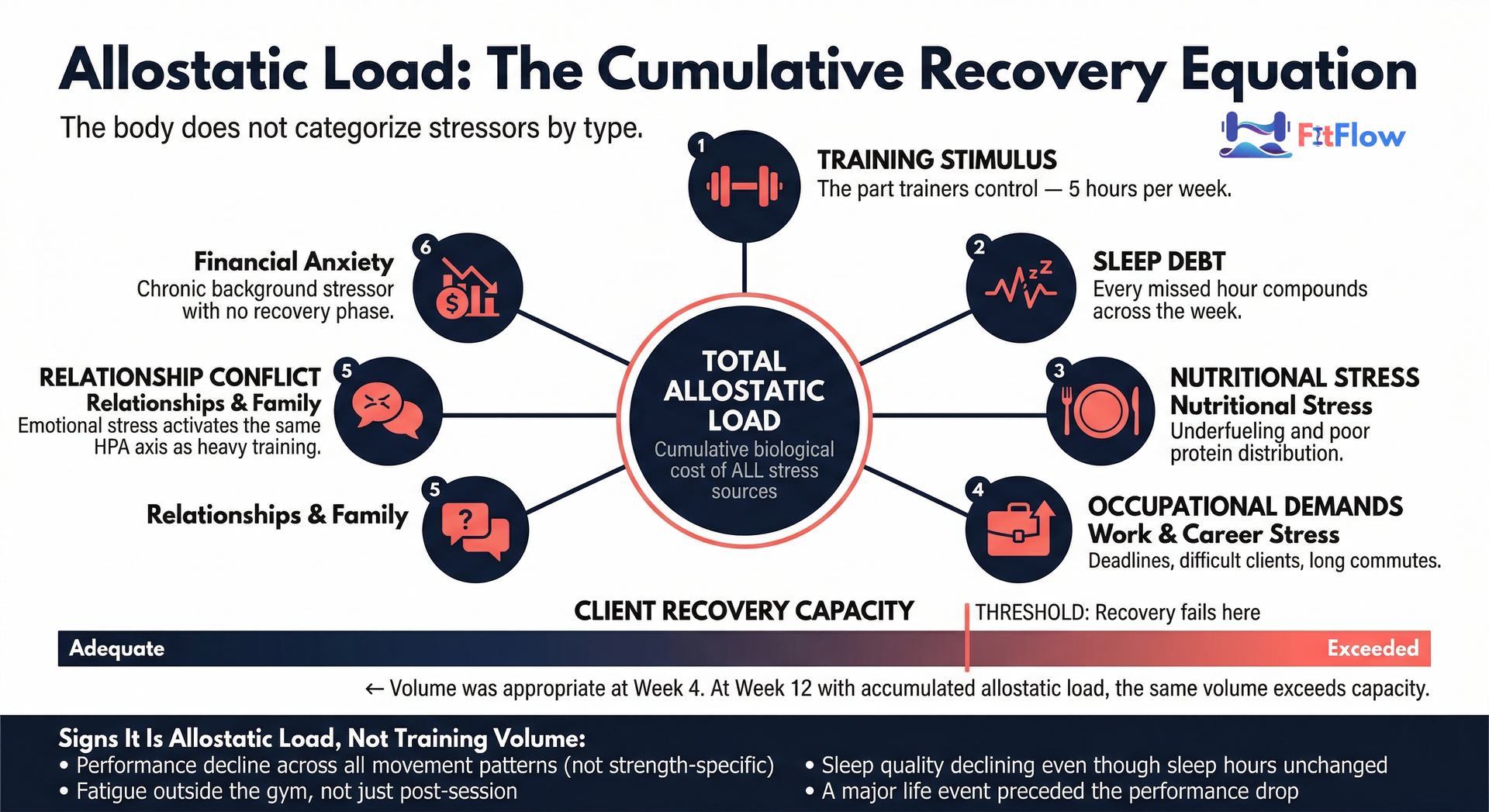
Allostatic load is the cumulative biological cost of chronic stress from all sources — training stimulus, sleep debt, nutritional stress, occupational demands, relationship conflict, financial anxiety, social obligations. The concept was first defined by McEwen and Stellar (1993) and has been applied to exercise contexts in recent research from Frontiers in Physiology (2025). The body does not categorize stressors by type. A client's divorce and a deadlift PR compete for the same finite recovery resources.
This is why the cortisol conversation, while culturally useful, is incomplete. Cortisol is one hormone in one component of the stress response. Allostatic load is the total burden across all stress systems — endocrine, immune, cardiovascular, metabolic. A client can have normal cortisol and still have elevated allostatic load from the compound effect of moderate sleep debt, moderate work stress, and moderate training volume stacking together.
Personal training intake forms typically assess fitness history, goals, and injury status. Almost none assess life stress load as a programming input. The result: trainers program volume for a rested, low-stress theoretical client while the actual client manages a cumulative load that renders the same volume excessive.
A client sleeping 6 hours per night with a high-stress job and relationship conflict has a fundamentally different recovery capacity than their baseline metrics suggest. Volume that was appropriate 8 weeks ago may break recovery at week 12 — not because training volume increased, but because allostatic load quietly accumulated. This is the same mechanism that causes hypertrophy programs to stall at 6 weeks — cumulative stress load exceeds recovery capacity, and the program takes the blame.
A single 1-10 stress rating at session check-in captures the symptom but not the accumulated load. Structured assessment works better: "Rate your work stress, relationship or family stress, and financial stress 1-10 separately." A client who rates work stress 8, family stress 7, and financial stress 6 does not have a "7 stress day." They have a compounding load crisis.
HRV provides an objective proxy — sustained suppression below personal baseline is one of the most reliable indicators of elevated allostatic load, even when clients report feeling "fine."
The programming implication: a trainer who understands allostatic load adjusts session intensity to match the client's actual recovery capacity that day — not their theoretical capacity. This is autoregulation, and it applies to every training modality. Recovery impairment is compounded in GLP-1 client populations, where lean mass preservation requires especially deliberate recovery programming.
Signs That Allostatic Load Is the Problem (Not Training Volume)
These are the diagnostic indicators that allostatic load — not programming — is the primary failure vector:
Life event preceded performance decline: The client was performing well, then a new job, relationship strain, or illness preceded the downturn. Training did not change. Recovery capacity did.
Performance decline is diffuse, not specific: Not isolated to one lift or muscle group — a general decline in energy, motivation, and work capacity. Systemic overload, not muscular fatigue.
Fatigue extends beyond the gym: The client feels "more tired than usual" throughout the day, not just after sessions. Life fatigue bleeding into training is allostatic load.
Sleep quality declining despite stable duration: Still sleeping 7-8 hours but waking unrefreshed — a hallmark of stress-disrupted sleep architecture.
Hidden Barrier 3: The Nutrition Myths Your Clients Believe (And That You Have Not Corrected)
Trainers are not registered dietitians, but they are the primary nutrition educators for most clients. The information gap between current evidence and common client belief is directly in trainer scope to close. What trainers fail to correct, clients continue to practice — and some of those practices actively impair recovery.
Myth 1: The 30-Minute Anabolic Window
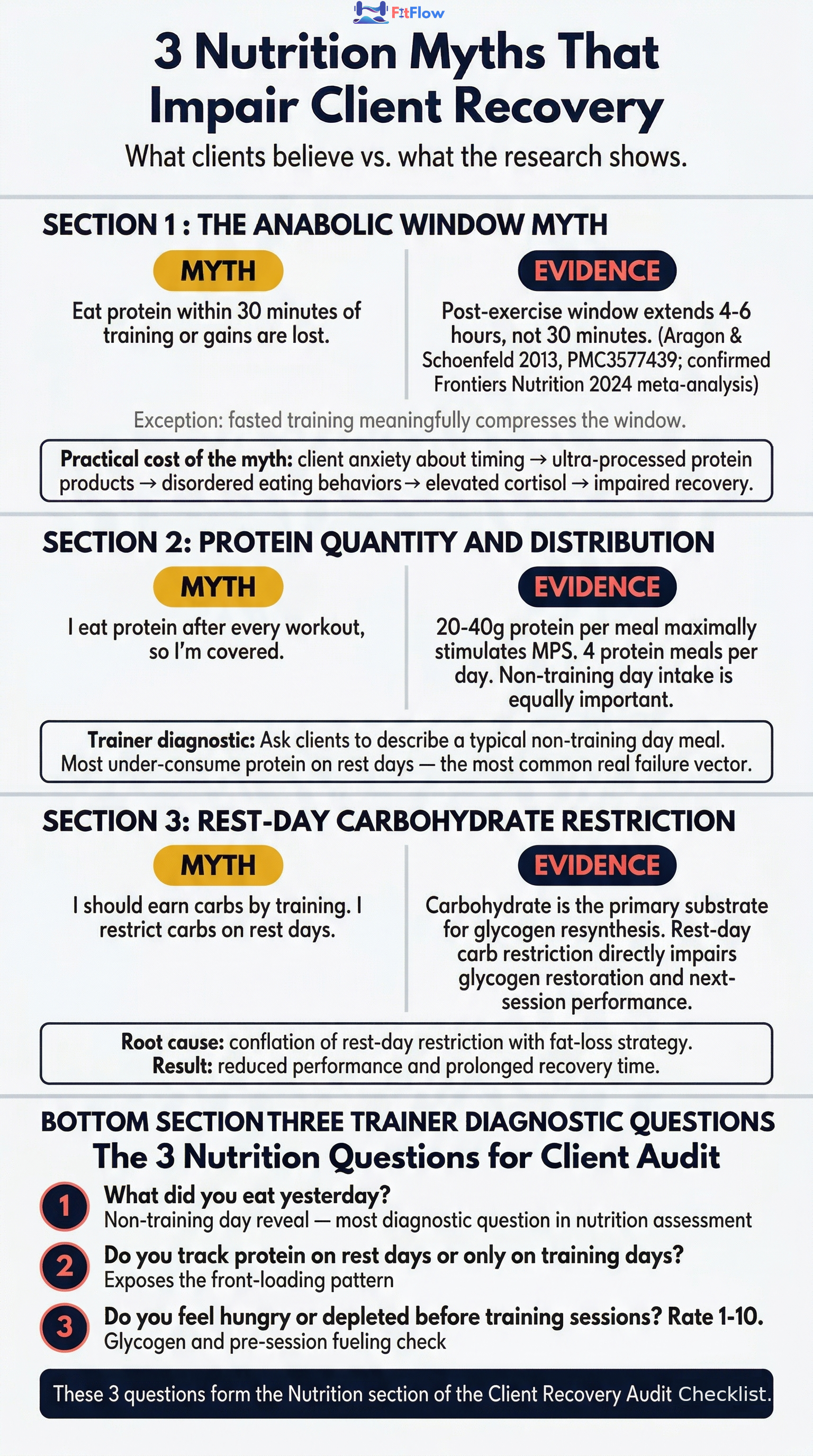
The belief: "I must eat protein within 30 minutes post-workout or my gains are lost." The evidence: the post-exercise anabolic window extends to 4-6 hours, not 30 minutes (Aragon and Schoenfeld, 2013; confirmed by a 2024 Frontiers in Nutrition meta-analysis). The only meaningful exception is fasted training, where the window is compressed because the body enters the session without a pre-exercise amino acid pool.
The cost: clients who believe the 30-minute window is critical resort to ultra-processed protein products, develop anxiety around meal timing that elevates cortisol, and neglect the more important variable — total daily protein intake.
Myth 2: Protein Quantity Is Sufficient If You Hit Your Daily Target
The real failure vector is distribution, not timing. Research shows 20-40g of protein per meal maximally stimulates muscle protein synthesis, and 4 protein meals per day is a practical target. Many clients who report "eating enough protein" are front-loading it post-workout and under-consuming through the rest of the day — especially on non-training days. Protein on rest days fuels repair from the previous session. Under-consuming on those days cuts recovery short.
Myth 3: Carbohydrates Are Optional on Rest Days
Carbohydrate is the primary substrate for glycogen resynthesis. Clients who carb-restrict on rest days impair the glycogen restoration that fuels the next session. Low-carb rest day culture is partly fueled by the belief that you should "earn" carbohydrates by training. This delays recovery and reduces next-session performance.
For the full evidence-based nutrition protocol — including specific protein distribution targets, carbohydrate timing by training type, and supplementation research — see our Evidence-Based Nutrition & Recovery Guide.
The 3 Questions to Uncover Nutrition Gaps on Non-Training Days
"What did you eat yesterday?" (Ask this on a training day, so "yesterday" was a rest day. This is the most revealing probe. Clients are rarely aware of how different their rest-day nutrition looks from their training-day patterns.)
"Do you track protein on rest days, or only training days?" (Most clients who track macros only do so on training days. Rest-day protein under-consumption is one of the most common and most correctable recovery failures.)
"Do you feel hungry or depleted before your training sessions? Rate it 1-10." (A consistently high rating suggests glycogen depletion from inadequate rest-day carbohydrate. The fix is nutritional, not motivational.)
Hidden Barrier 4: Volume Creep Is Silent. Deloads Are Rare. This Is Why Clients Hit Walls.
Volume creep is the gradual, unplanned accumulation of training volume without corresponding deload periods. It is the most common structural programming failure in general fitness personal training — nearly invisible until it manifests as plateau, injury, or a client who quits.
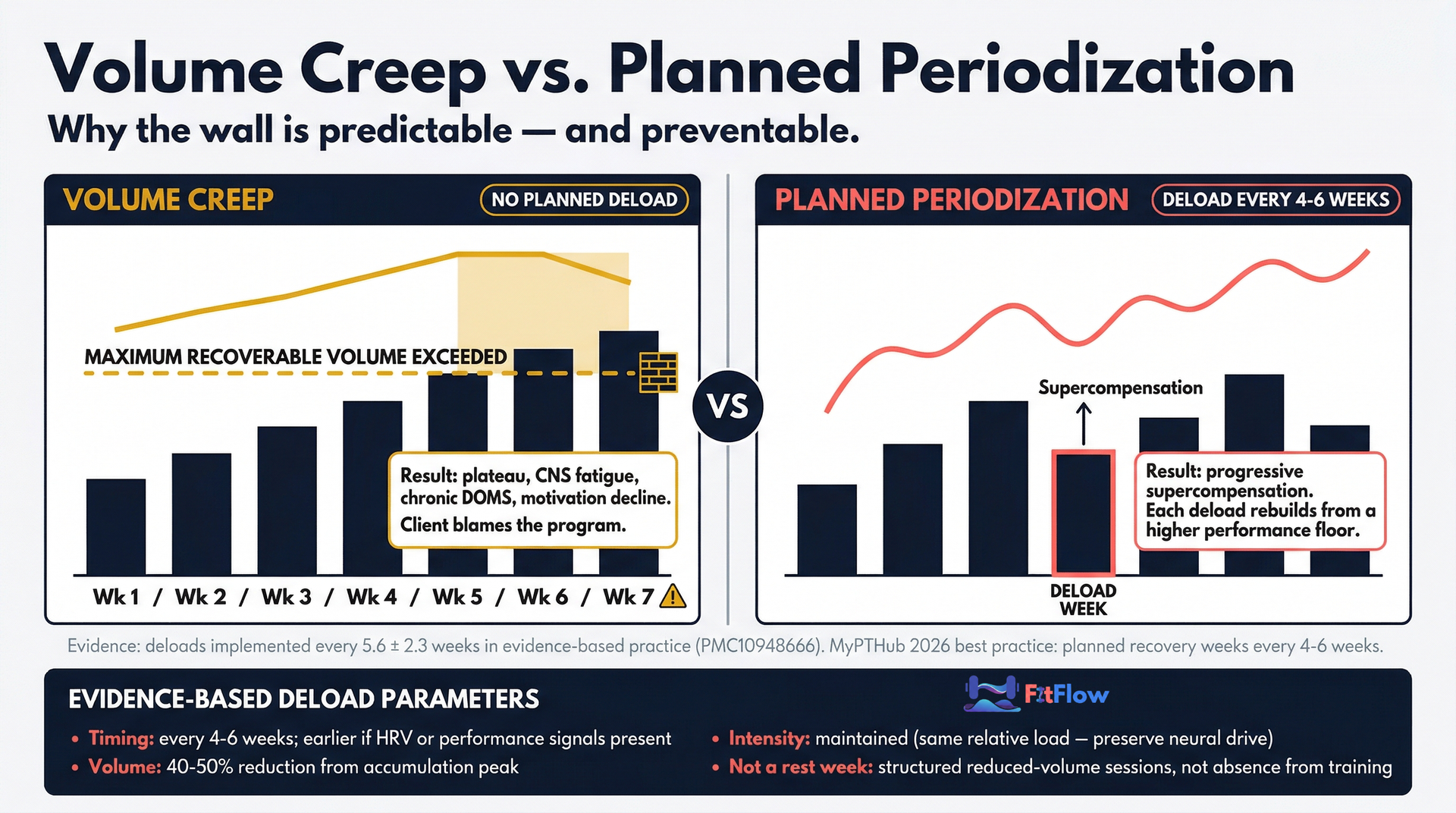
Most strength and physique practitioners implement deloads every 5.6 plus or minus 2.3 weeks (PMC10948666). MyPTHub 2026 cites planned recovery weeks every 4-6 weeks as baseline. Many trainers with general fitness clients do not implement formal deloads — they rely on "life deloads" (missed sessions, holidays) that are unplanned and insufficient.
Why do trainers avoid deloads? Three reasons, all psychological:
Client perception: "I'm paying for training and you want me to go easy?" Trainers fear that deload sessions read as insufficient value — a perception problem, not a programming problem.
Trainer identity: Progressive overload as a professional signal. Adding weight, reps, and sets demonstrates visible coaching competence. Reducing volume feels like retreat.
Outcome ambiguity: Deload sessions do not produce visible gains. Their contribution to long-term progress is invisible to clients — which means their absence goes unnoticed until the consequences arrive.
The consequences accumulate silently:
Cumulative CNS fatigue: Without planned deload, neural fatigue compounds until it manifests as plateau, injury, or motivation collapse.
Chronic DOMS: Clients who never fully recover between accumulation phases develop permanent baseline soreness — persistent tissue damage they normalize.
Plateau misattribution: Clients blame the program. Trainers blame commitment. The real issue is absent recovery structure.
Evidence-based deload parameters for most training clients:
Timing: Every 4-6 weeks, or earlier if fatigue indicators are present
Volume reduction: 40-50% of normal training volume; intensity maintained at the same relative load to preserve neural drive
Not a rest week: Deloads are structured, reduced-volume training sessions — not absence from the gym
Autoregulated triggers: Sustained HRV suppression below baseline, 2 or more consecutive sessions with declining performance, 3 or more days of persistent DOMS, or client-reported motivation decline
The reframe for client communication: "A deload week is not a rest week. It is a supercompensation accelerator. Your body gets stronger during recovery, not during training. A deload lets the adaptation catch up to the stimulus you have already provided."
How to Program Deloads Without Losing Client Trust
Trainers who introduce deloads proactively — explaining them during the first session — report less client resistance than those who introduce them after fatigue has set in.
A practical structure: 3 weeks of progressive accumulation followed by 1 week at 50% volume. Explain at onboarding: "Week 4 is your body's growth week. The first 3 weeks provide the stimulus. Week 4 is when adaptation happens." Frame the deload as the payoff, not the pause. For how periodized deload structure integrates into long-term programming, see our evidence-based program design guide.
Hidden Barrier 5: You Have a Recovery Data Stream. You Are Not Reading It.
Almost 50% of U.S. adults now own a fitness tracker or smartwatch (Everfit 2026). An increasing proportion of your clients arrive at sessions with HRV data, readiness scores, and sleep quality metrics on their wrists. They are already measuring their recovery. The question is whether you are integrating that data into programming decisions.
Heart rate variability (HRV) measures the variation in time between heartbeats, regulated by the autonomic nervous system. High HRV = parasympathetic dominance = adequate recovery. Low HRV = sympathetic dominance = stress/fatigue state. It is among the most sensitive non-invasive recovery biomarkers available (MDPI Sensors 2026, PMC12787763; PMC11204851).
The practical protocol for integrating HRV into trainer programming decisions uses RMSSD (root mean square of successive differences) — the standard HRV metric for recovery assessment:
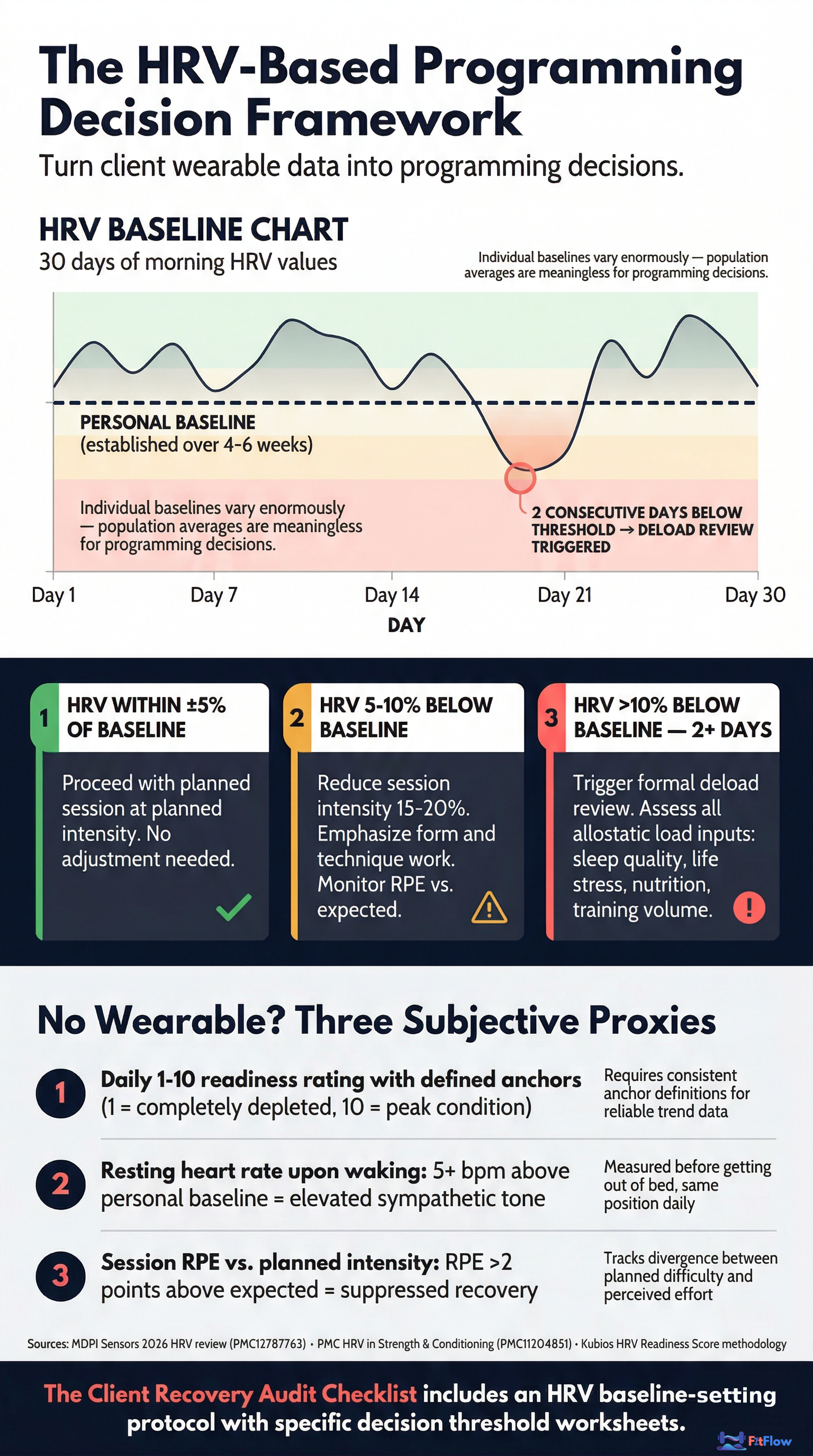
Establish a personal baseline: Have the client measure RMSSD daily upon waking, same position, same device, for 4-6 weeks. Individual baselines vary enormously. Population averages are meaningless for programming individual clients.
Apply decision thresholds:
HRV within plus or minus 5% of personal baseline: proceed with the planned session as programmed
HRV 5-10% below baseline: reduce intensity. Emphasize form work, technique refinement, or lower-intensity variations of planned movements
HRV more than 10% below baseline for 2 or more consecutive days: trigger a formal deload review. Assess allostatic load. Something in the 163 hours has shifted
Check exercise timing: The WHOOP/Nature study showed that high-intensity workouts within 2 hours of bedtime produce a 32.6% decrease in overnight HRV. If a client's morning HRV is chronically suppressed without apparent cause, ask about exercise timing before assuming a recovery pathology.
Build HRV and readiness score tracking into your client dashboard alongside performance and body composition data. The data stream already exists. The missing piece is integrating it into programming decisions.
How Many of Those Hidden Barriers Apply to Your Client? Audit Them Now. Download the Audit Checklist.
What to Do If Your Client Does Not Have a Wearable
Not every client owns an HRV-capable device. Three subjective proxies approximate readiness without technology:
Anchored 1-10 readiness rating: Define what each number means (1 = "cannot complete warm-up," 5 = "normal training day," 10 = "best in months"). Anchored ratings produce far more useful data than unanchored self-reports.
Resting heart rate upon waking: A sustained increase of 5+ bpm above baseline suggests elevated sympathetic tone and suppressed recovery.
Session RPE vs. planned intensity: If RPE 7 sessions consistently feel like RPE 9, recovery is not matching training demands. An overshoot of 2+ points sustained over multiple sessions is a meaningful fatigue signal.
Putting It Together: The Client Recovery Assessment Framework
What separates trainers who systematically produce results from those who do not is not programming sophistication — it is assessment depth. The 5 barriers above are all assessable. None require advanced technology. All require asking better questions and treating answers as programming inputs.
A structured client recovery audit covers 7 domains:
Sleep timing and architecture: Training day vs. rest day patterns, consistency, quality rating, exercise timing relative to bedtime
Allostatic load: Work stress, relationship/family stress, and financial stress assessed separately — not as a single composite rating
Nutrition patterns on non-training days: Protein distribution, carbohydrate intake, and hydration practices when the client is not actively training
Training block structure: Deload frequency, volume accumulation rate, and whether volume creep has been assessed
Wearable data integration: HRV baseline status, readiness score usage, and whether the data informs programming decisions
Hydration and electrolyte balance: Often the most under-assessed mechanical recovery variable, especially in clients who train in heated environments or at altitude
Client compliance and accountability systems: Whether recovery protocols are tracked, communicated, and integrated into the client's training plan — not just prescribed and forgotten
When to conduct the audit: At intake for all new clients. Triggered when any client shows 2+ consecutive weeks of declining performance, persistent soreness, or motivation decline. Repeated quarterly as life stress patterns change.
You will spend 5 hours per week with your client. They will spend 163 hours managing the recovery capacity that determines whether those 5 hours produce results. Your job is to understand both.
Recovery Failure Is Predictable. Your Response Should Be Too.
Recovery failure is not random. It has predictable causes, and most are within the trainer's diagnostic and programming control.
The barriers identified here — inadequate sleep architecture assessment, unrecognized allostatic load, persistent nutrition myths, absent deload structure, and unread wearable data — are not extraordinary failures. They are the baseline errors that occur when trainers optimize training without auditing recovery.
The 2026 fitness industry has already moved. Recovery monitoring is core scope. You are not just a fitness professional. You are a recovery manager for the 163 hours you are not with your clients.
The asymmetry is simple: the program your client does not recover from will not produce results. The program they do recover from — even if it is less impressive on paper — will. Build the recovery system first.
This article is the diagnostic layer — identifying what trainers miss. To build the complete recovery system, start with our Evidence-Based Nutrition & Recovery Guide (sleep protocols, nutrition timing, supplementation evidence, hydration targets). For the systems-level view, see why your training program is not the problem — your system is.
Recovery Failure Is Not Random. It Has 7 Diagnosable Causes. Get the Free Recovery Audit.