Elite Coaches Are Not Better at Programming. They Are Better at Deciding.
You have 34 clients on your roster. One of them, call her Client A, intermediate, training with you for 14 months, has stopped progressing. You have three plausible interventions on the table: add a working set, tighten her RIR from 3 to 2, or address the 6.2-hour average sleep she mentioned in her last check-in. Each intervention is defensible. You know what each one does. You do not know which one to use first. You pick two of them at the same time, see something change in week 3, and cannot tell which variable moved the needle. The next plateau will require the same guess.
That moment, knowing what to do but not knowing what to do first, is usually not a knowledge problem. It is a decision problem. And it is where a lot of competent coaches get stuck. They know the levers. They just do not have a clean way to choose the first one.
Elite coaches are not magically better at exercise prescription. They are better at decision triage. Their decision tree is smaller and less dramatic. It tells them what to look at, what to ignore for now, and when to change one variable instead of three. That is not less coaching. It is what keeps coaching sane when you have 35 clients and every check-in is trying to become its own little investigation.
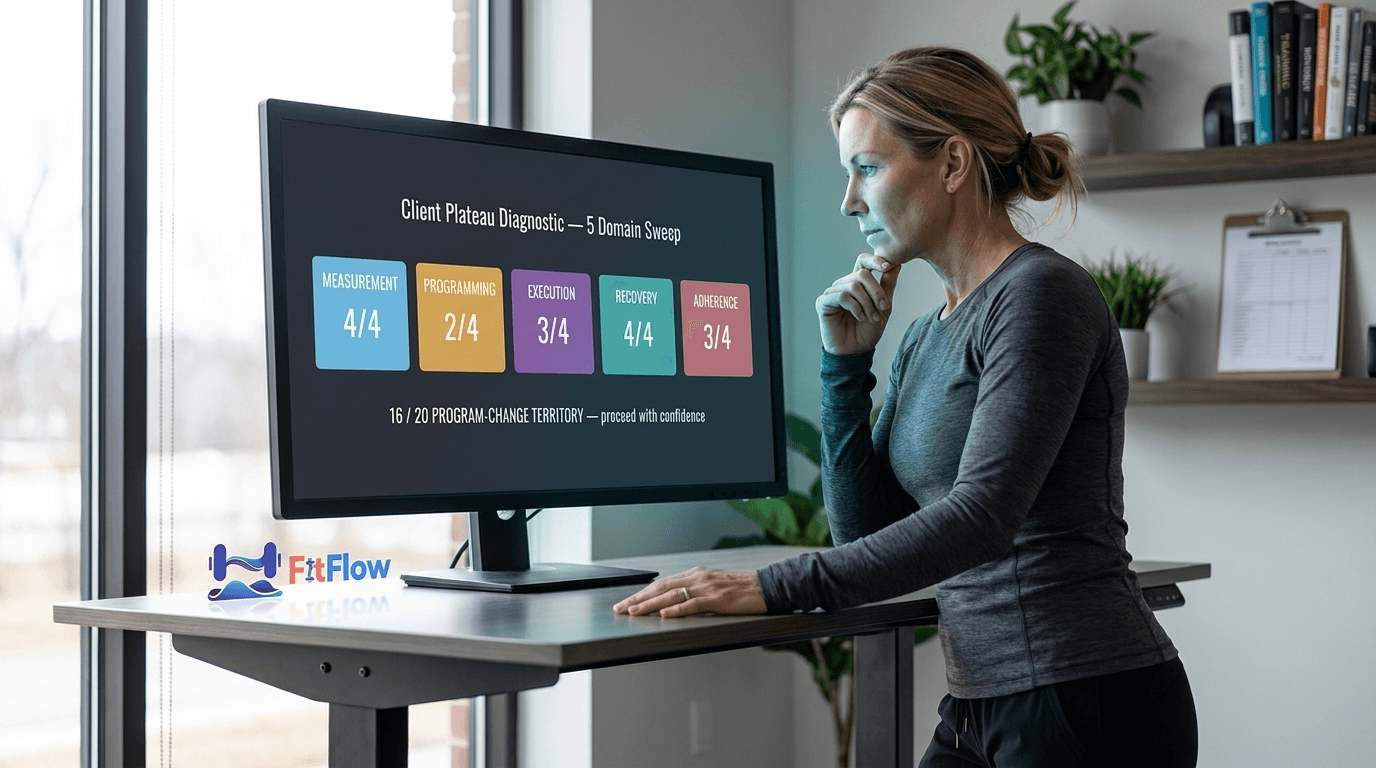
Decision triage in coaching means reducing all possible interventions to the one best next move for this client, right now. You apply that move, watch what happens, and only then reconsider. The term borrows from medical triage, where the hard part is not knowing every treatment. It is deciding what gets attention first when time, energy, and certainty are limited. The rest of this article is what that looks like with a 35-client book.
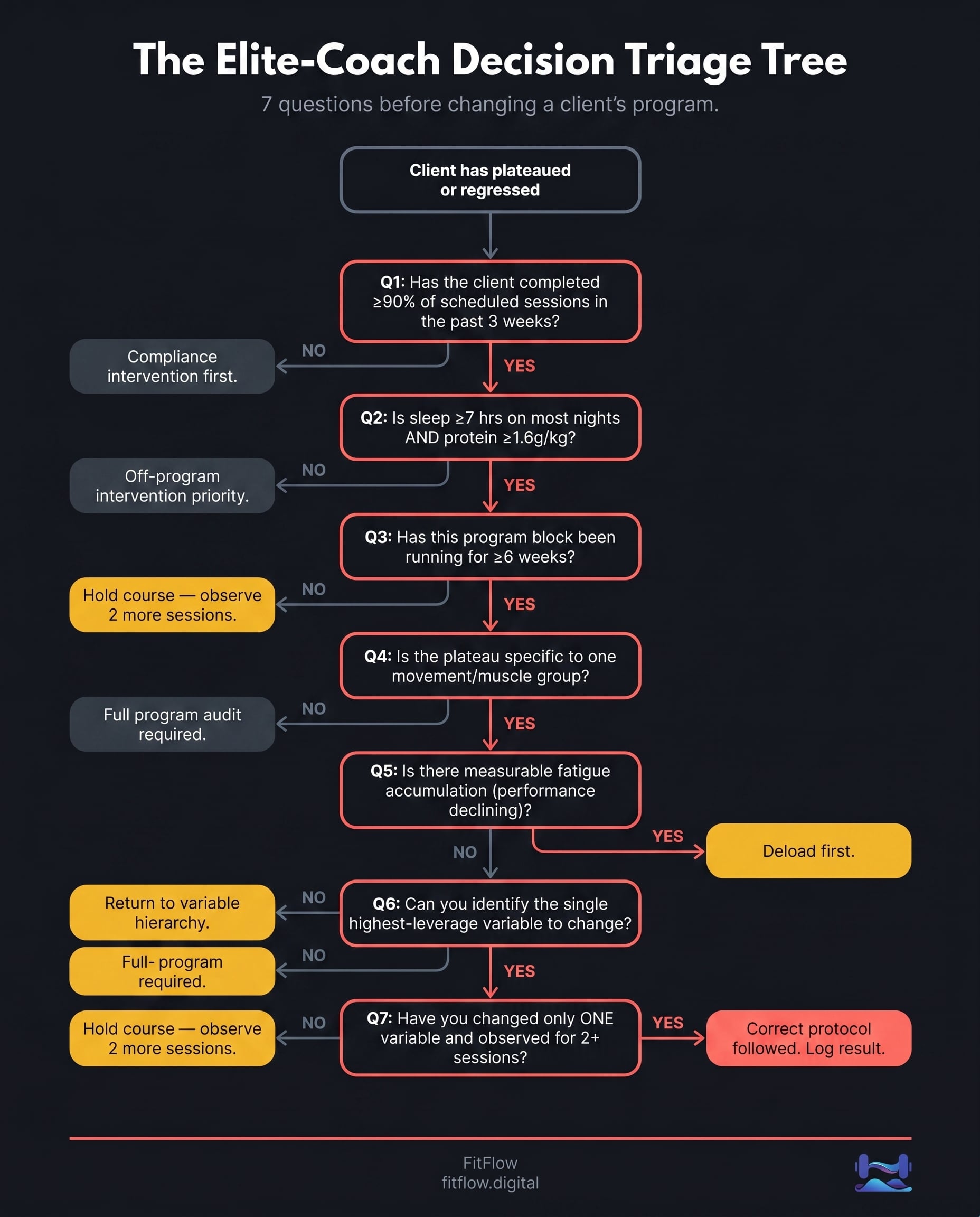
We built the Elite-Coach Decision Triage Card, a 7-question protocol for the moment a client plateaus and you have to decide what changes. Available at the end of this article.
This is not the 80/20 of training variables. We covered the variable hierarchy that feeds the decision tree in a separate post. That post ranks which levers carry the most weight on average. This post is one layer above it. The 80/20 tells you which lever matters in general. Decision triage tells you which lever matters for Client A, at Week 14, when two of them are equally valid and you have to pick one.
The knowledge is not the problem
Most trainers know more than they can use
The evidence-based training world has produced a generation of coaches with more programming knowledge than any group before them. Sam, the composite scaling trainer this post is written for, has read Helms. He uses RIR. He knows MEV, MAV, and MRV by heart. He listened to Iron Culture on the drive in this morning. He can probably quote the ACSM 2026 Position Stand on failure proximity well enough to annoy someone at dinner.
And he still sometimes does not know what to do first.
The ceiling is not knowledge. The gap is between knowing all the variables and having a process for choosing between them in real time, for a specific client, without second-guessing yourself 72 hours later. Brad Schoenfeld, the most-cited resistance training researcher of the past decade, has said for years that resistance training responses vary widely between people [1]. The same program can produce different outcomes in different clients. The coach who can read that individual signal has an edge that another paper, by itself, will not give them. Reading the signal is a decision skill. It needs a process.
For the evidence base behind this, see our evidence-based program design pillar guide. Elite coaches do not have secret science. They use the same evidence base. They just route decisions through it more cleanly.
The science gives you variables. It does not make the call.
The 2025 Sports Medicine dose-response meta-regression (Schoenfeld, Krieger, Pelland, Nuckols et al.; 67 studies, 2,058 participants) put numbers on the diminishing returns curve: each set above 12.25 per muscle group per week adds about 0.24% additional hypertrophy [2]. That helps with "how much volume?" It does not answer the annoying real-world version: should this client, in this week, with this recovery status, get more volume right now?
That second question is a decision. It needs a process.
The 2025 Frontiers in Psychology framework on coaches' decision-making (Kolar et al.) says the same thing in a more academic register. Session-level and program-adjustment decisions depend on domain expertise and pattern recognition, not an algorithm that spits out the answer [3]. The better coach does not always know more. Often, they rule out the irrelevant options faster.
That is the point here. Sam already has the variables. What he needs is routing.
Get the 7-question card for deciding what to change first. Most coaching mistakes happen when you change three things at once and cannot tell what worked. This card gives you the 7 questions to run before changing a client's program, so you can pick one variable, set an observation window, and make the next decision cleaner. Get the Triage Card.
What decision triage actually means
Triage is about sequence
Medical triage prioritizes which patient to treat first. Not based on what the doctors know, but on urgency, severity, and available resources under time pressure. The doctors already know what to do for each patient individually. The triage question is sequencing under constraint.
Elite coaches use the same kind of skill. When a client shows a plateau, a compliance problem, or a performance regression, the first move is not to throw knowledge at it. The first move is to ask: what is the one intervention most likely to matter, and what change will let me read the result without muddying the signal? Then they apply that, and only that.
The thing that wrecks this is the multi-variable response: changing load and volume and sleep advice in the same week. The client improves. Great. Now what worked? Nobody knows. The next plateau requires the same guess. The Helms, Valdez, and Morgan Muscle and Strength Pyramids framework [4] is useful here because it gives priority order: adherence first, then volume and intensity, then frequency, then exercise selection. The pyramid is not a buffet. It is a hierarchy.

Why better coaches often change less
The instinct under uncertainty is addition. If something is not working, do more of something. Add a set. Add a deload. Add a nutrition protocol. I get the urge. It feels useful. At scale, though, it mostly creates noise. With 35 clients, the multi-variable response is not a better coaching decision. It is a harder one to learn from.
The Sports Medicine 2024 N of 1 methodology paper (Atkinson et al.) made the principle explicit. To detect a true individual response signal versus measurement noise, researchers must hold all other variables constant and repeat the intervention at least twice [5]. The same logic applies to coaching decisions. The coach who changes one variable has a readable result. The coach who changes three has a confounded one.
Better coaches change less because that is how you actually learn what works for a specific client. Each clean intervention adds a data point. Each muddy intervention hides the lesson.
The 2025 PMC network meta-analysis on autoregulated resistance training [6] reinforces the point from a different angle. Autoregulated systems (APRE, RPE-based prescription, RIR-driven programming) outperform percentage-based prescription precisely because they build decision responsiveness into the protocol itself. The coach is not handing out a fixed load. They are handing out a decision rule. That rule produces better strength outcomes than rigid prescription.
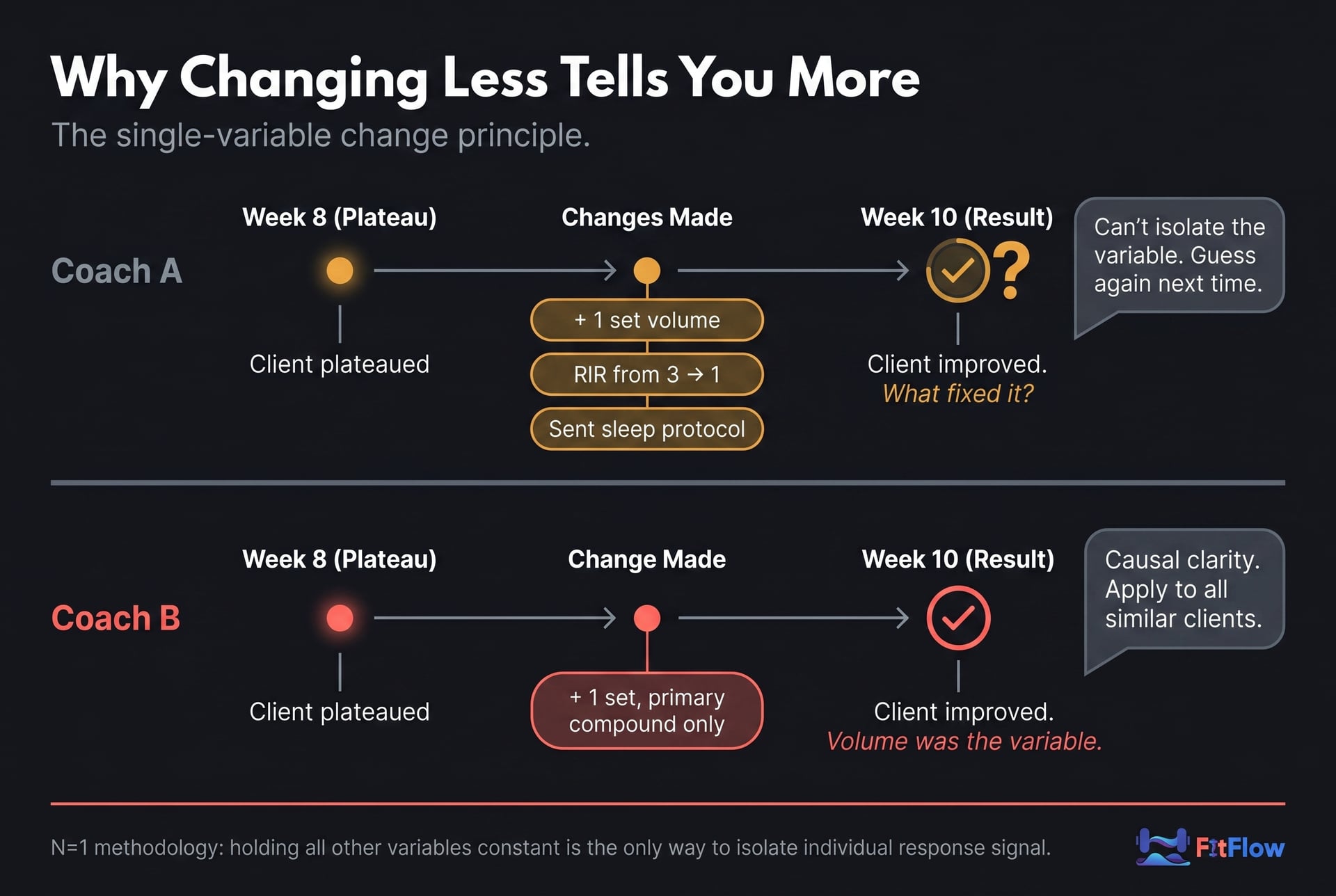
Two coaches. Same client. Same plateau at Week 8.
Coach 1 adds a set, shortens rest intervals, and emails over a nutrition checklist. The client reports a small improvement at Week 10. Coach 1 cannot tell which intervention did it. Was it the volume? The density? The protein bump? Coach 1 keeps all three changes in place because removing any of them feels risky.
Coach 2 asks first: is she recovering? Sleep is averaging 7.4 hours. Compliance is 92% over the past month. Protein is 1.7 g/kg. The plateau is real. Coach 2 adds one set to the primary compound. Week 10: the plateau resolves. Coach 2 knows exactly what fixed it. She also knows the next thing to try if it had not.
Same knowledge. Cleaner decision.
The 3-question triage protocol
This is the process. Run the same three questions in the same order, even when the client presents the problem in a messy way. Especially then. The questions are the spine of the lead magnet at the end of this article. The order matters.
Question 1: is this a program problem or an off-program problem?
Every coaching decision starts with the same question: where is the constraint? Before any program variable is adjusted, the elite coach establishes whether the plateau is inside the program (insufficient stimulus, wrong overload variable, structural error) or outside it (sleep deprivation, life stress, nutritional deficit, compliance gap, illness recovery).
Most coaches skip this question. They adjust the program because the program is the part they control. But a sleep-deprived client who gets 4 more sets per week is just receiving more stress on top of a recovery deficit. The adjustment may be defensible on paper. It is still the wrong first move.
The diagnostic check is three items. Run them in order, every time:
Compliance: has the client completed at least 90% of scheduled sessions in the past 3 weeks?
Recovery: is sleep at or above 7 hours on most nights, by self-report?
Protein: is intake at or above 1.6 g/kg of bodyweight per day? Morton et al.'s 2018 meta-analysis of 49 studies established that threshold as the dose-response ceiling for resistance-training adaptation [7]. Below it, hypertrophy is meaningfully impaired regardless of how clean the program is.
If any of these is "no," the off-program variable takes priority. Do not adjust the program. The decision routes to the off-program audit methodology, which is Branch 1 in the next section.
For the full taxonomy of why clients stop progressing, see the client diagnostic post. And when the problem is delivery rather than programming, your training program is not the problem; your system is is the next stop.
Question 2: if it is a program problem, what is the one variable?
If Question 1 rules out off-program causes, the coach moves to the program. Question 2 forces single-variable selection, not multi-variable brainstorming. This is where most coaches lose the discipline.
The variable hierarchy. Use this sequence:
Progressive overload mechanism. Has the right dimension of overload been applied for this client's training age and plateau type? Load? Volume? Density? ROM? Tempo? Effort/RIR? See the overload variable spectrum that branches the decision tree for the 6-dimension breakdown.
Structure. Is the program structurally sound? Frequency, split, primary movements, session design? See the structural baseline elite coaches start from before they triage.
Stimulus-fatigue balance. Is the client at or near maximum recoverable volume? Is a deload indicated? Mike Israetel's RP Strength volume landmarks (MEV, MAV, MRV) are the practitioner reference here [8]. They are decision points, not equal-weight thresholds.
Exercise selection. Last. Only if the first three have been checked and ruled out. See what to fix before rotating exercises.
The elite coach does not begin with exercise selection. They end there, if they reach it at all.
A worked example. Client B, intermediate, 3 years training. Bench press has stalled for 3 weeks. Sleep and nutrition checked clean (Q1). Coach 2 checks Q2. Is load the right lever? The client is operating at 2 RIR on most sets. There is no headroom to add load safely without form breakdown. Volume is sitting at 12 sets per week, near MAV. Density check: rest intervals are at 90 seconds on the working sets. The coach extends rest to 120 seconds. Session quality immediately improves. Load progresses the following week. No exercise was changed. No volume was added. One variable moved.
That is the protocol doing its job.
Question 3: after the change, how long will you watch?
The third question disciplines the coach, not the client. How long will you observe the result of the single-variable change before reconsidering it?
Elite coaches set an observation window: minimum 2 sessions, typically 3. This constraint is what makes single-variable changes readable. If the result has not emerged within the window, return to Question 2 and select the next most useful variable. Do not stack a second variable on top of the first one before the window closes.
Mike Tuchscherer's Reactive Training Systems framework is the practitioner reference here. RPE-based autoregulation is not a free-for-all. It is a decision rule applied at every session, with the observation window providing the feedback loop [9]. Tuchscherer has put it directly: well-designed systems make good decisions easier. The observation window is a piece of system design that makes the decision easier next time.
This is also the question coaches drop when the client is impatient. Or when they are impatient themselves. Both sides want to layer in another change before the window closes. That impulse is the problem. The observation window is not a delay. It is what makes the next decision better than the last one.
The five decision branches
The triage protocol can send you to five places. That is the point. You do not want to re-derive the whole logic every Monday morning while 12 check-ins are waiting. You want a small set of branches that tell you what kind of problem you are dealing with.
Turn the 5 branches into a 90-second check-in tool. The article explains the decision branches. The card gives you the routing system. Pull it up before a plateaued client check-in, answer the 7 questions in order, and know whether to address compliance, recovery, overload, fatigue, structure, or exercise selection. Download the Decision Card.
If you want a single-page version of these five branches and the 3-question protocol that routes to them, printable and designed to live next to your check-in workflow, the Elite-Coach Decision Triage Card is below. It puts the seven questions that drive the protocol in one place, with the five branches mapped on the back.
Branch 1: the off-program branch
When Question 1 sends you here, address the off-program variable first and leave the program alone. The priority order is simple: sleep below 7 hours, high life stress, protein below 1.6 g/kg, then training compliance. A client completing 70% of sessions does not need a clever hypertrophy adjustment yet. They need enough consistency for the program to show its actual effect. For the complete off-program audit methodology, the methodology post walks the full sequence with intervention scripts.
Branch 2: the overload branch
When Question 2 sends you here, pick one overload dimension. For an intermediate client, start with effort/RIR if the client has been living above 3 RIR and can tighten to 2. Then consider volume, with one added working set if MRV headroom exists. Then density, if rest periods are the limiter. Then load, if training age and current performance support it. Zourdos et al.'s validation of the RIR scale at r=0.88-0.91 reliability in trained lifters [10] is what makes effort a measurable progressive variable rather than guesswork.
Branch 3: the stimulus-fatigue branch
When Question 2 sends you here, accumulated fatigue is probably blurring the signal. The giveaway is erratic performance: one good session, one poor session, repeated week after week. That is not a clean plateau. That is fatigue noise. The intervention is a structured deload: reduce volume by 40-60%, hold load, run it for one week, then re-enter at the starting volume of the previous mesocycle with a load progression. Coaches catch this faster when they track session performance instead of staring only at body composition metrics. For the metrics elite coaches actually track and why hypertrophy programs plateau at 6 weeks, the cluster has the deeper treatment.
Branch 4: the structural branch
When Question 2 sends you here, the program itself is the constraint. Structural problems show up across sessions, not as one awkward lift on one bad day: frequency too low for a muscle group, sessions too short to approach MEV, push/pull balance off, accessory work crowding out the primary work. The fix is a redesign, not a little variable tweak.
Branch 5: the exercise selection branch
This is the last branch, reached only after Branches 1 through 4 have been checked and ruled out. Better coaches change exercises less often because most plateaus are not exercise-selection problems. If you reach this branch, you have already checked recovery, overload, fatigue, and structure. Then, yes, change the exercise. Do it deliberately, and set an observation window. Random rotation is exactly what this branch is trying to stop.
The most common decision errors
Every error below comes from skipping the protocol, running it out of order, or abandoning it mid-window. Sam will probably recognize at least one from his last six check-ins. That recognition is useful. Not as a client diagnosis, but as a coach diagnosis.
Error 1: changing multiple variables at once
This is probably the most common coaching error. When a client plateaus, the multi-variable response feels thorough. It signals effort and care to the client, and it calms the coach's own anxiety. In practice, it makes the result unreadable.
Name the pattern honestly. If your last program change adjusted load, volume, exercise selection, and sleep advice in the same week, you did not make a clean coaching decision. You made a guess. The correction is one variable per adjustment cycle. The next plateau can teach you something, but only if the previous adjustment was readable.
A scenario from a coach in our network with a 38-client book. The client plateaus on bench. The coach adds a set, drops rest from 90 to 75 seconds, and tells the client to hit 1.8 g/kg protein. Three weeks later, the bench is up 2.5 kg. The client asks what worked. The honest answer is, "I don't know. Probably the volume. Maybe the rest change. Maybe the protein. Could be all three." That is not coaching at scale. That is coaching inside a fog.
Error 2: going to exercise selection first
The second common error is exercise variation. Sometimes the client is bored. Sometimes the coach is bored writing the same movement pattern again. Novelty can create a short-term bump, but it can also hide the actual problem. Two mesocycles later, the same plateau returns because exercise selection was never the constraint.
The priority inversion is the failure. Exercise selection is the last decision branch, not the first. A coach who defaults to exercise rotation when a client plateaus is operating without a triage protocol. They have a reflex. For the exercise selection discipline that prevents this, the deeper post is the next read.
Error 3: skipping Question 1
The third error. Adjusting the program without first checking off-program variables. A client averaging 5.5 hours of sleep per night who receives an additional 4 sets per week will not adapt at the same rate as a fully recovered client. The program adjustment is not technically wrong. It is poorly timed.
The cost is not the wasted set. The cost is that the program adjustment burns a coaching decision window, the observation window from Q3, on a client who cannot express the adaptation. The result is ambiguous. The coach learns nothing. The client continues to plateau. Three weeks were spent on data that does not generalize.
Elite coaches treat Question 1 as mandatory, not optional. The check is structural, not situational. They run it even when the client is not complaining about sleep or nutrition, because the absence of complaint is not evidence of adequacy.
What better coaches already have in place
The triage protocol needs a base to sit on. Good coaches usually build three things before they ever reach the decision moment. Sam probably has most of this in place already. Naming it makes the dependency visible.
A structural program baseline
Better coaches do not triage from scratch. They start with a sound baseline: defined frequency, split, primary movements, and progression model. The decision tree stays small because the obvious structural issues have already been handled. The protocol assumes the foundation is sound. It does not rebuild it every week. For the structural baseline elite coaches start from before they triage, the structural reference post lays it out.
A variable hierarchy they already know
The variable hierarchy from the 80/20 post (adherence, progressive overload, protein at 1.6 g/kg, sleep at 7+ hours, exercise consistency over 8-12 weeks) is the knowledge base the protocol runs on. Coaches need to know which variables tend to matter most across the population. Then the triage protocol applies that ranking to one client. The ranking tells you what to consider. The protocol tells you which one to pull right now. For the variable hierarchy that feeds the decision tree, the prioritization post is the companion read.
A metric system that reads the signal
Better coaches track the data that helps them decide. Not body weight every day. Not DOMS scores as if soreness were a moral achievement. Session RPE, sets completed versus prescribed, top-set load per primary movement, weekly volume per muscle group, and compliance rates over rolling 3- and 6-week windows. These metrics feed Questions 1 and 2 directly. Without them, the coach is operating on memory and anecdote. With them, the protocol can run in minutes per client. The Iron Culture and MASS Research Review community has been making this case for years [11]: individualization runs on data, not feel.
Scaling the decision system
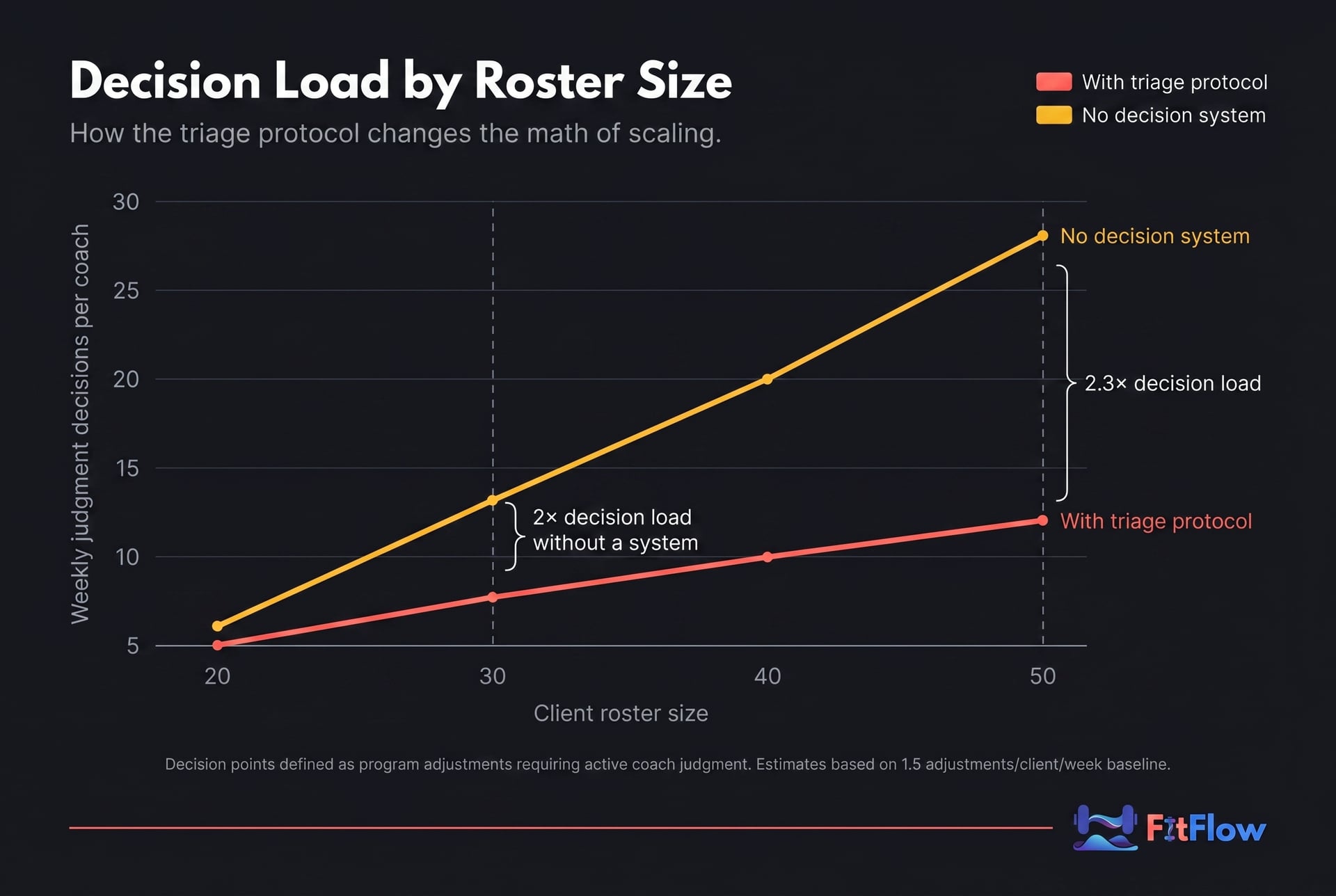
At 5 clients, an idiosyncratic decision process is sustainable. At 35 clients, it is not. The coach who reinvents the decision process for every client plateau is not scaling. They are replicating a bespoke cognitive burden 35 times per week and calling it personalization.
The decision system scales because it repeats. Same 3 questions. Same order. Same 5 branches. Same observation window. Decision time per client drops because the coach is not inventing a fresh process every time. Jonathan Goodman's Scaling Coaching work for the PTDC has documented this dynamic [12]: coaches who reach capacity and then stop growing often have not reduced per-client decision overhead. They add clients and cognitive burden in equal proportion until the business is capped by the coach's mental bandwidth, not market demand. The triage protocol changes that ratio.
The Building the Elite editorial cluster from January 2026 makes a similar systems argument [13]: intelligent structure beats outcome-focused shortcuts. A decision process is structure. Reactive variable changes are shortcuts. The difference compounds across the book.
The AI-coaching question that Mike Israetel and the RP Strength cluster have been pressing on for the past 18 months [14] lands here too. As platforms add readiness flags, progression alerts, and automated check-in prompts, the coach's role gets clearer. AI can flag a plateau. It cannot fully understand the cause in context. It can surface a signal. The human coach still has to decide what to do with it.
FitFlow's client management system is built around exactly this routing problem. The platform surfaces the signals that feed Questions 1 and 2 in the triage protocol (compliance rates, session performance trends, check-in flags) so the decision is fast and grounded in current data, not memory. See how FitFlow supports the decision system at scale on the pricing page, or explore the tools that use the decision framework across clients on the features page.
Use the same triage protocol on your next client plateau. The card includes the 7-question triage sequence, the single-variable rule, the observation-window check, and the decision flow for common plateau scenarios. Built for coaches managing 20-50 clients who need cleaner decisions without re-reading a full article before every check-in. Get the Free Triage Card.
Closing the loop
The gap between competent and elite is not always what you know. Often, it is how you decide. A smaller decision tree, one that triages before it intervenes, changes one variable instead of three, and observes the result before reconsidering, makes coaching easier to learn from. That is the whole point. Experience only compounds when the decisions are readable.
For Sam, with 35 clients and a solid evidence base, the plateau is not knowledge. It is decision routing. The 3-question triage protocol makes the knowledge he already has more consistent across the book.
For Amanda, with 10 clients and a fresh certification, this is not a catch-up tool. It is the habit to build early. Multi-variable guessing is a bad reflex, and it gets harder to unwind once it becomes normal.
The Elite-Coach Decision Triage Card puts the 7 core questions in a single-page format you can use at every client check-in. Run it every time a client plateaus, hits a compliance gap, or surfaces ambiguous data. Download it below.
Frequently Asked Questions
Comments