The Most Ignored Factor in Client Results: Why Daily Step Consistency Predicts Outcomes More Than Anything You Program

The number on your client's wrist you've never used
Your client just texted you. They are frustrated. They have been doing every workout you assigned. Their protein is on point. Their sleep, by their self-report, is "fine." And the scale has not moved in three weeks.
You scroll your training app. You check their lift PRs. You scan their macro log. Everything you can see looks correct. The variable that actually explains their plateau is sitting on the wrist they used to send you that text, and you have never opened it.
It is their daily step count. NEAT, non-exercise activity thermogenesis. The movement they accumulate when you are not watching them train.
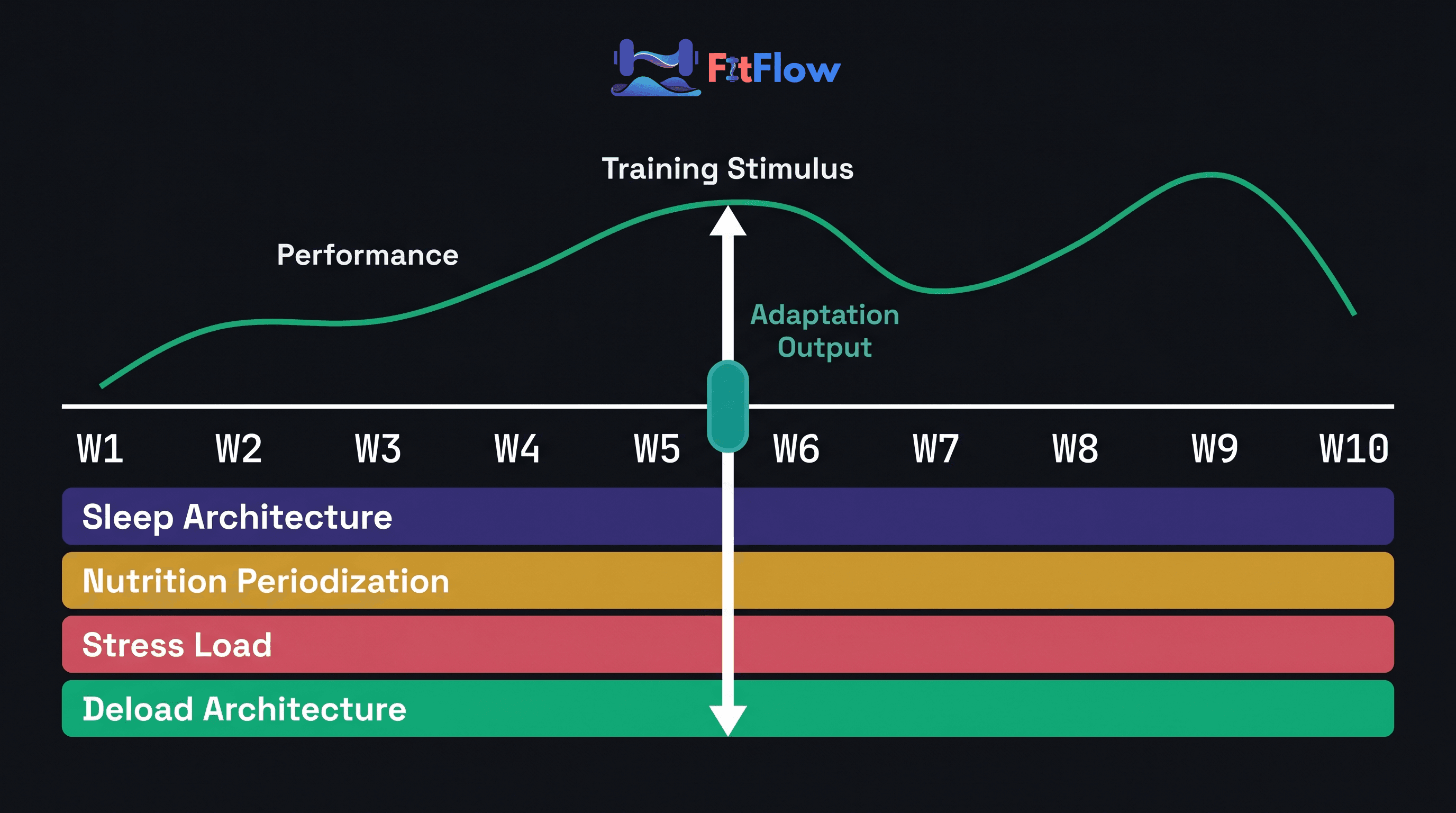
This is not a side note. Differences in NEAT between people of similar body size can reach 2,000 kcal/day [Levine, 2002, Best Practice & Research Clinical Endocrinology & Metabolism]. A 10% body-weight reduction can drop daily energy expenditure by 20–25%, and roughly half of that drop comes from NEAT compensation, not BMR [Müller et al., 2015, Obesity Reviews; Hall, 2012, Obesity]. That is the uncomfortable part: the variable you do not measure may be moving more energy through your client's day than the workout block you wrote.
Most trainers optimize the variables clients can see: sets, reps, macros, weights on the bar. Then they ignore the daily movement number that often explains why the plan works for one client and stalls for another. It is sitting on your client's wrist right now, and you probably have not looked at it.
Half your clients already own the device that measures it. Zero of them have a trainer-grade protocol for what the number means.
Get the diagnostic tool while you read. Download "The Ignored Variable Audit: 12-Point NEAT Diagnostic Checklist for Trainers", a printable client-intake tool that turns daily step data into a coaching decision in under 15 minutes. Get the free checklist ->
The timing matters. This week, May 12-15, 2026, the European Congress on Obesity (ECO 2026) is meeting in Istanbul. One session abstract covers an 18-trial, 3,758-participant meta-analysis on daily steps during nutritional lifestyle programs, published in the International Journal of Environmental Research and Public Health. The finding: people who maintained roughly 8,500 daily steps during weight loss and 8,241 steps during maintenance had better long-term weight-maintenance outcomes after dieting [Daily Steps During Nutritional Lifestyle Modification Programs, 2026, Int J Environ Res Public Health / ECO 2026]. Not 10,000. Not "move more." Around 8,500.
This article covers the evidence, the reasons trainers miss the step trend, and the protocol you can use in a normal weekly check-in. No new certification. No 40-minute lifestyle consult. Just one number most clients already track.
What the data actually shows
NEAT deserves more attention for three plain reasons: it is large enough to matter, easy to measure, and easier to sustain than most planned exercise.
Effect size. NEAT can vary by up to 2,000 kcal/day between people of similar body size [Levine et al., 1999, Science; Levine, 2002]. For context, 2,000 kcal/day is roughly the maintenance intake of a small adult. A client averaging 4,200 steps and a client averaging 11,000 steps can look identical on paper: same training, same food log, same starting body composition. Their results may still split hard. The 1999 Science paper from the Mayo Clinic group found the lean cohort spent roughly 152 more minutes per day standing and moving. That is not a willpower variable. It is a pattern you can measure.
Compliance. A 2015 Mayo Clinic Proceedings review of NEAT versus structured exercise (EAT) concluded that structured exercise has poor compliance despite heavy promotion, while NEAT has stronger long-term adherence [Villablanca et al., 2015, Mayo Clinic Proceedings]. At the coaching level, that matters more than it sounds. A behavior that can be built in 60-90 second chunks has a different survival rate than a fourth weekly cardio session. Most clients will not keep that extra cardio block for 18 months. Many will keep an extra 2,500 steps per day.
Operating threshold. The ECO 2026 meta-analysis found that participants who increased daily steps to about 8,454 during weight-loss phases and maintained 8,241 during maintenance had better long-term outcomes and less regain [Daily Steps During Nutritional Lifestyle Modification Programs, 2026, Int J Environ Res Public Health]. The familiar "10,000 steps" target came from a 1960s Japanese pedometer campaign, not a controlled trial. For fat-loss clients, 8,500 is the better starting point.
Compensation. When a client enters a caloric deficit, NEAT can drop by 20-40%, a metabolic-adaptation mechanism documented by Müller et al. (2015) and modeled by Hall (2012). The client may be telling the truth when they say they are "following the plan." Their body is quietly reducing fidgeting, standing time, ambulation, posture shifts, and other incidental movement. Stiegler and Cunliffe (2006), reviewing energy-balance dynamics during weight loss in Sports Medicine, identified this compensation as a major reason some plateaus do not respond to program changes. Without monitoring, the drift is invisible. With monitoring, it becomes a useful weekly check-in signal.
The comparison below shows why NEAT outranks every other off-program variable a trainer can influence and why the math is decisive.
Off-Program Variable | Daily Caloric Range | Measurement Friction | Trainer Scope | Long-Term Adherence |
|---|---|---|---|---|
NEAT / Daily Steps | Up to ~2,000 kcal/day inter-individual range | Already on client's wrist | FULL (no Rx) | HIGH (Mayo, 2015) |
Sleep (within 6–9 hr range) | ~300–500 kcal/day appetite effect | Wearable-tracked, architecture is medical | LIMITED (hygiene only) | MEDIUM |
Hydration | ~50–150 kcal indirect via satiety | Self-report only | FULL | LOW (novelty effect) |
Stress / cortisol | ~100–400 kcal appetite-mediated | Indirect (HRV proxy) | LIMITED (mental health risk) | LOW |
Protein distribution | ~0 kcal direct (synthesis efficiency) | Self-report meal log | FULL | MEDIUM (food preference resistance) |
Alcohol | ~100–500 kcal direct caloric load | Self-report | FULL | MEDIUM–LOW |
The conclusion is uncomfortable for the standard intake form. Of the off-program variables a trainer can influence, NEAT has the largest caloric range, low measurement friction, a clean scope-of-practice fit, and strong long-term adherence. It should be on the intake form and in the weekly review.
For the comparative 7-variable ranking of all other non-training inputs, including sleep, protein distribution, alcohol, hydration, stress, and energy availability, see the sister analysis, Improve Results Without Changing Training - Run This Audit Instead. That hierarchy ranks NEAT first for the same reasons this article isolates it for depth. For the underlying caloric-balance and TDEE evidence base that contextualizes the compensation mechanism, see the comprehensive evidence base on caloric balance, TDEE, and recovery science.
Why trainers miss it
If NEAT predicts outcomes this well, why is it missing from so many intake forms and weekly check-ins? It is not because trainers are careless. The blind spots are built into how the profession teaches, measures, and rewards coaching.
Blind spot 1: trainer education focuses on the session
NASM, ACE, ISSA, NSCA, and ACSM core curricula heavily emphasize program design, exercise selection, biomechanics, and in-session output: form, load, RPE, tempo. Off-program movement, the 23+ hours per day your client is not with you, usually gets tucked into a "nutrition and lifestyle" module. Trainers leave certification ready for the 1-2 hours per week they see the client and underprepared for the 166+ hours they do not.
The fix is not a new certification. It is a single intake question, a phase-aligned target, and one weekly metric. Three sentences, embedded in your existing workflow.
Blind spot 2: the data looks too easy to value
Half your clients wear a Garmin, Apple Watch, Whoop, Fitbit, or Oura. The step count is auto-populated. There is no friction to access it. Wearable technology has been the #1 fitness trend in the ACSM Worldwide Survey of Fitness Trends for 20 consecutive years through 2026 [ACSM, 2026, Worldwide Survey of Fitness Trends]. The infrastructure is ambient.
That is part of the problem. Variables that took effort to produce, like a meal log, sleep journal, or HRV note, feel like data the trainer should respect. Passive data feels like background noise. The hidden rule becomes: if the client did not actively report it, I will not actively coach on it. That is backwards. The most useful behavioral data is often the data the client did not curate.
Blind spot 3: step counts feel too basic
"Just go for a walk" sounds like advice your aunt would give. Trainer culture tends to rank load-progressed compound lifts above incidental movement, structured cardio above unstructured walking, and prescribed protocols above lifestyle nudges. NEAT coaching can feel like the least professional intervention in the toolkit. That is probably why it gets ignored.
The 2026 wearable moment changes the framing. There is a wide gap between "walk more" and "your 7-day baseline is 4,200 steps; we are moving that toward 8,500 over six weeks because your phase requires it." The threshold plus the protocol is the professional intervention. NASM's 2026 Top Fitness Trends Report lists low-impact movement and micro-workouts among the year's emphases [NASM, 2026, Top Fitness Trends Report]. The field is catching up to the evidence, slowly.
Blind spot 4: plateaus trigger program changes first
When a client plateaus at week 4-8 of a deficit, the reflex is to change the program: add a workout, increase volume, drop calories. A better first move is to check whether the hidden inputs changed before you change the visible ones. NEAT compensation in a deficit can show up as a 20-40% downward drift over 4-8 weeks [Müller et al., 2015; Hall, 2012]. That is not a guess. It is a documented adaptation.
If you change the program before you check the step trend, you are likely treating a NEAT compensation problem with a programming change. The intervention is mismatched to the bottleneck. This is the same failure pattern named in the Smart Training cluster's system over plan thesis: the program was not the bottleneck; the measurement system around it was. The same logic governs nutrition adherence in the parallel adherence-systems framework and recovery in the diagnostic deep-dive into the 5 hidden recovery barriers. NEAT is the off-program variable that the same systems lens isolates.
These blind spots are not character flaws. They are defaults baked into trainer education, wearable data habits, and trainer culture. The protocol below is meant to make the better behavior easier than the default one.
The NEAT diagnostic protocol
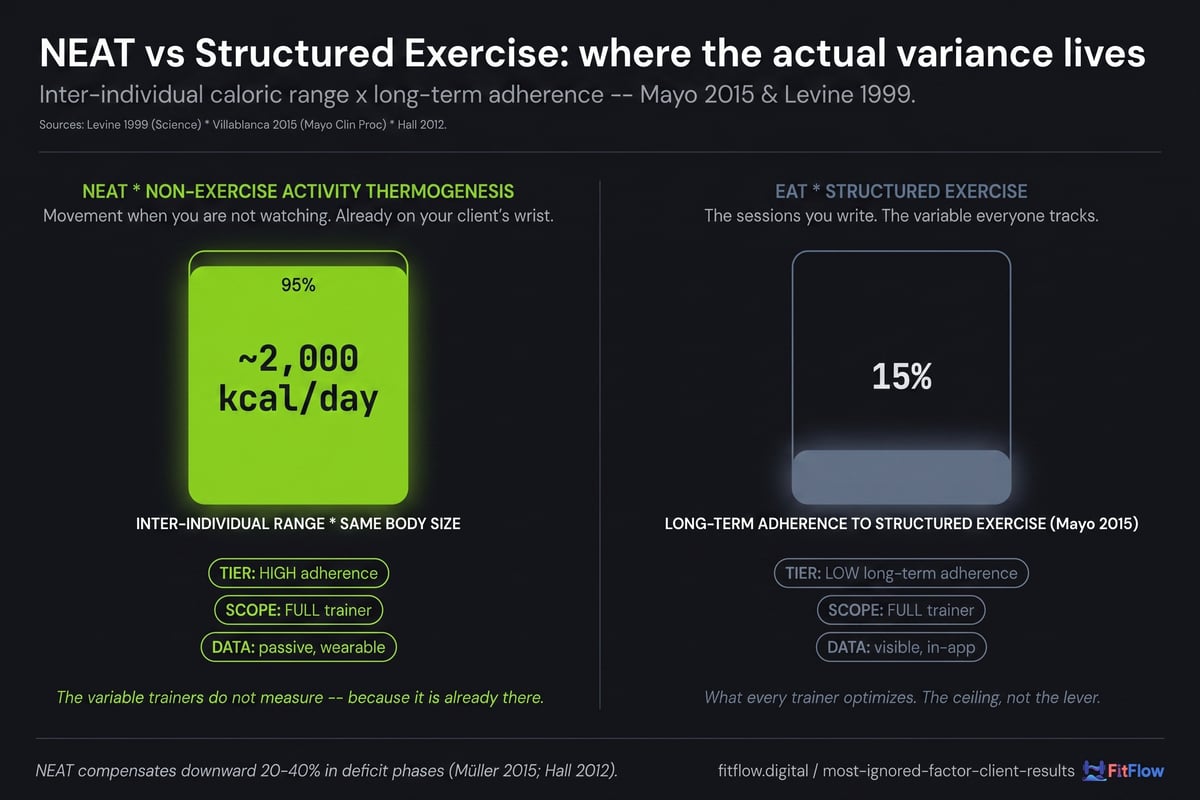
Diagnostic protocols only work if they are short enough to run when Monday gets messy. This one has five measurements: three at intake, two recurring weekly. Total trainer time per client: 8-12 minutes at intake, then about 90 seconds per weekly check-in.
Intake measurement 1: 7-day rolling baseline
Before recommending a step target, capture the client's current 7-day average step count from their wearable or phone health app. This is the rolling baseline. Most clients will report a daily target, usually something like "I try to hit 10K," but their actual 7-day average is often lower, commonly 4,000-6,500. The gap between perceived and actual is useful by itself. Never set a target without the baseline.
If the client does not own a wearable, a 7-day phone-tracked step average is acceptable for baseline establishment. Smartphones systematically under-count by ~10–15% versus dedicated wearables [PMC12628992, 2025, on wearable step-count accuracy], but the trend is what matters, not the absolute number.
The most useful onboarding sentence: "Before I prescribe anything, I need to know what your baseline looks like. Send me a screenshot of your 7-day step trend from your Health app or watch."
Intake measurement 2: phase-aligned target
Set the step target based on the client's current programming phase, not a generic 10K default. The phase-aligned targets below derive from the ECO 2026 8,500-step anchor for fat loss and the Tudor-Locke pedometer step-category framework [Tudor-Locke et al., 2009, Sports Medicine], which classifies <5,000 as sedentary, 5,000–7,500 as low active, 7,500–10,000 as somewhat active, 10,000–12,500 as active, and >12,500 as highly active.
Body-composition / fat-loss phase: 8,500-10,000 steps/day floor (ECO 2026 anchor).
Maintenance / recomp phase: 7,500-8,500 steps/day.
Hypertrophy / mass-gain phase: 6,500-8,000 steps/day, intentionally lower to preserve energy availability for adaptation.
Strength / athletic performance: 7,000-9,000 steps/day, with attention to fatigue and training quality.
GLP-1 medication client: protected 7,000-step floor (see GLP-1 section below).
The phase-aligned target eliminates the "10K for everyone" generic recommendation that fails high-volume hypertrophy clients by stealing adaptation energy and under-doses fat-loss clients because 8K is below the ECO 2026 threshold.
Intake measurement 3: lifestyle constraint audit
Five quick questions:
Average daily occupational sitting time (desk-bound vs. mobile work)?
Commute type (car, transit, walk/bike)?
Household responsibilities involving movement (childcare, pets, errands)?
Wearable accuracy assumption (Garmin and Apple Watch are most accurate; Fitbit and Whoop slightly variable; phone is least)?
Any planned travel, life disruptions, or recovery from injury in the next four weeks?
These five answers tell you whether the target is realistic or whether the client needs friction-reduction ideas: walking calls, treadmill desks, walking meetings, lunchtime walks. Frontiers in Public Health (2022) documents workplace NEAT interventions as more durable when they match the person's environment instead of being blanket-prescribed [Frontiers in Public Health, 2022, NEAT in the Workplace].
Weekly measurement 4: 7-day average and trend direction
At each weekly check-in: 7-day average step count plus trend direction (rising, stable, falling). The trend is the diagnostic signal. A single low day is noise; a 3-week declining trend is the bottleneck.
The 90-second protocol is simple: the client screenshots their 7-day step trend, or your client-management software pulls it automatically. You check three things: 7-day average versus target, trend direction, and any week with a >25% deviation from baseline as a life-event flag. Bonomi et al.'s secondary analysis of the Step-Up Trial (PMC5970037) identified daily step pattern, not single peak days, as the variable most associated with weight-loss success. Pattern beats peak. The 7-day rolling average makes that usable.
Weekly measurement 5: adherence-outcome correlation
Cross-reference the weekly step trend against the outcome metric: weight, body composition, or performance. If steps are at target and the outcome is stalled, NEAT is not the bottleneck; escalate to the next-most-likely variable (sleep, protein distribution, stress load), referenced via the 7-variable Off-Program Leverage Hierarchy. If steps are below target and the outcome is stalled, NEAT is the bottleneck; intervene there before changing any other variable.
That is the full diagnostic loop. Five inputs. Two of them recurring. The trainer time cost is roughly 90 seconds per client per week. The outcome leverage is the single largest off-program variable on the board.
Companion tool. These 5 measurements map directly to the 12-Point NEAT Diagnostic Checklist. Use it to run the audit in 12 minutes per client, with scoring keyed to the threshold table below. Get the free checklist ->
The NEAT threshold table
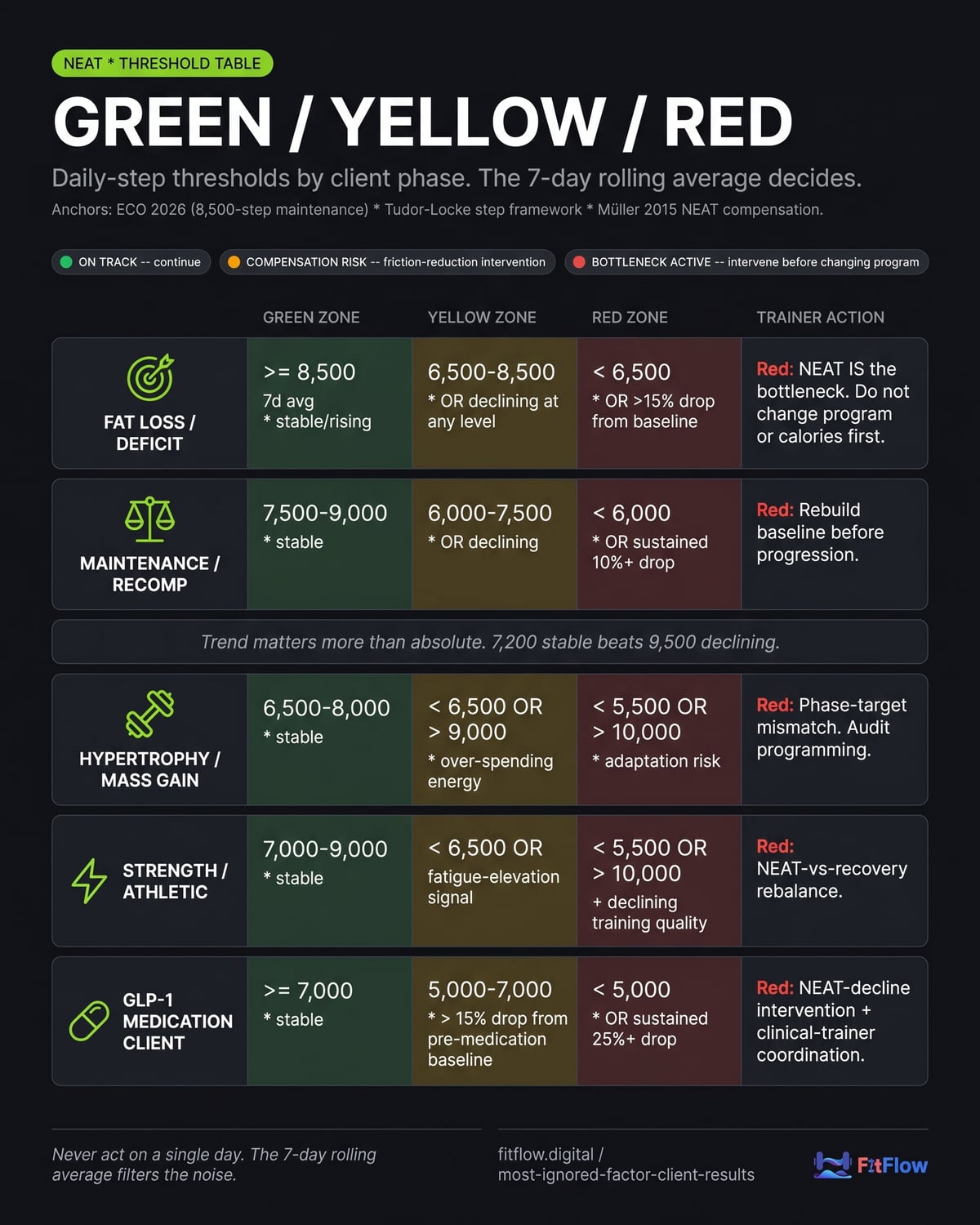
Thresholds turn raw step data into a coaching decision. Use these operating ranges across phases. Adjust within ±500 steps for individual constraints, but keep the trend-direction logic intact. The trend can matter more than the absolute number.
Client Phase | Green Zone (On Track) | Yellow Zone (Compensation Risk) | Red Zone (Bottleneck Active) | Trainer Action |
|---|---|---|---|---|
Fat Loss / Deficit | ≥8,500 7-day avg, stable or rising | 6,500-8,500 7-day avg, OR declining trend at any level | <6,500 7-day avg, OR >15% drop from baseline | Green: continue. Yellow: friction-reduction (walking call, lunchtime walk). Red: NEAT is the bottleneck; intervene before changing program or calories. |
Maintenance / Recomp | 7,500-9,000, stable trend | 6,000-7,500 OR declining trend | <6,000 OR sustained 10%+ drop | Green: continue. Yellow: check life-constraint changes. Red: rebuild baseline before progression. |
Hypertrophy / Mass Gain | 6,500-8,000, stable trend | <6,500 OR >9,000 (over-spending energy) | <5,500 (chronic under-movement) OR >10,000 (energy-availability risk for adaptation) | Green: continue. Yellow: adjust per direction. Red: phase-target mismatch; audit programming. |
Strength / Athletic | 7,000-9,000, stable trend | <6,500 OR fatigue-elevation signal | <5,500 OR >10,000 with declining training quality | Green: continue. Yellow: monitor fatigue. Red: rebalance NEAT and recovery. |
GLP-1 Medication Client | ≥7,000, stable trend | 5,000-7,000 OR >15% drop from pre-medication baseline | <5,000 OR sustained 25%+ drop | Yellow: structured 10-minute movement scaffolding. Red: NEAT-decline intervention with clinical-trainer coordination (see GLP-1 section). |
Two interpretation rules matter more than the exact cutoff:
Trend matters more than absolute. A client at 7,200 steps stable for six weeks is in a stronger position than a client at 9,500 declining 800/week. The trend is the signal; the absolute is context.
Never act on a single day. Single-day deviations are noise: illness, travel, weather, a meeting that ran long. The 7-day rolling average filters the noise. Acting on one day is the most common early-protocol mistake.
This table is where the protocol becomes a decision. The intake measurements feed into it. The weekly check-in references it. The case study below shows the difference between tracking the number and guessing around it.
Put the threshold table to work this week. Download "The Ignored Variable Audit: 12-Point NEAT Diagnostic Checklist for Trainers", the printable companion that scores each client against the table in under 15 minutes. Get the free checklist ->
Two clients, one trainer, two outcomes
Same trainer. Same 12-week fat-loss program. Same starting body composition. Same training-session adherence (both clients completed 32 of 36 sessions). Same self-reported nutrition adherence (~80%). Different outcomes. Only one variable differed: NEAT.
Client A: the invisible bottleneck
Week 0 baseline: 5,800 7-day average steps. Desk-bound office worker. Daily commute by car. The trainer set "10,000 steps as a goal" verbally at intake but did not measure the baseline or track weekly.
Week 4: scale stalled. Trainer added two cardio sessions per week. The step trend, not tracked, had drifted to ~5,200.
Week 8: scale still flat. Trainer reduced caloric intake by 200 kcal. Step trend at ~4,800. NEAT compensation was in full effect. The deficit deepened, the unconscious movement reduction deepened with it, and the program kept being adjusted around a variable nobody was measuring.
Week 12: the client lost 1.4 kg total. They reported, "I was hungry the whole time and the scale barely moved." They did not renew the package.
Client B: the diagnostic protocol
Week 0 baseline (measured): 5,400 7-day average steps. Similar desk-bound profile. The trainer set a phase-aligned target of 8,500 with a 4-week ramp (+800 per week) and tracked weekly via app integration.
Week 2: 7-day avg = 6,800. Yellow zone with a rising trend. Continue.
Week 4: 7-day avg = 8,100. Green zone, rising. Scale −1.1 kg. On track.
Week 8: 7-day avg = 8,700. Green zone, stable. Scale −2.4 kg cumulative. Programming unchanged.
Week 12: 7-day avg = 8,500. Green zone. Scale −3.8 kg cumulative. Client renewed.
Outcome comparison
Metric | Client A (No NEAT Protocol) | Client B (NEAT Protocol) |
|---|---|---|
Baseline 7-day steps | Not measured | 5,400 |
Week 12 7-day steps | ~4,800 (estimated) | 8,500 |
Step delta over 12 weeks | −1,000 (NEAT compensation) | +3,100 (protocol-driven) |
Total weight change | −1.4 kg | −3.8 kg |
Programming changes | Added cardio, reduced kcal | None |
Client satisfaction | Did not renew | Renewed |
Trainer time on program adjustments | ~45 min over 12 weeks | ~12 min over 12 weeks (NEAT check-ins) |
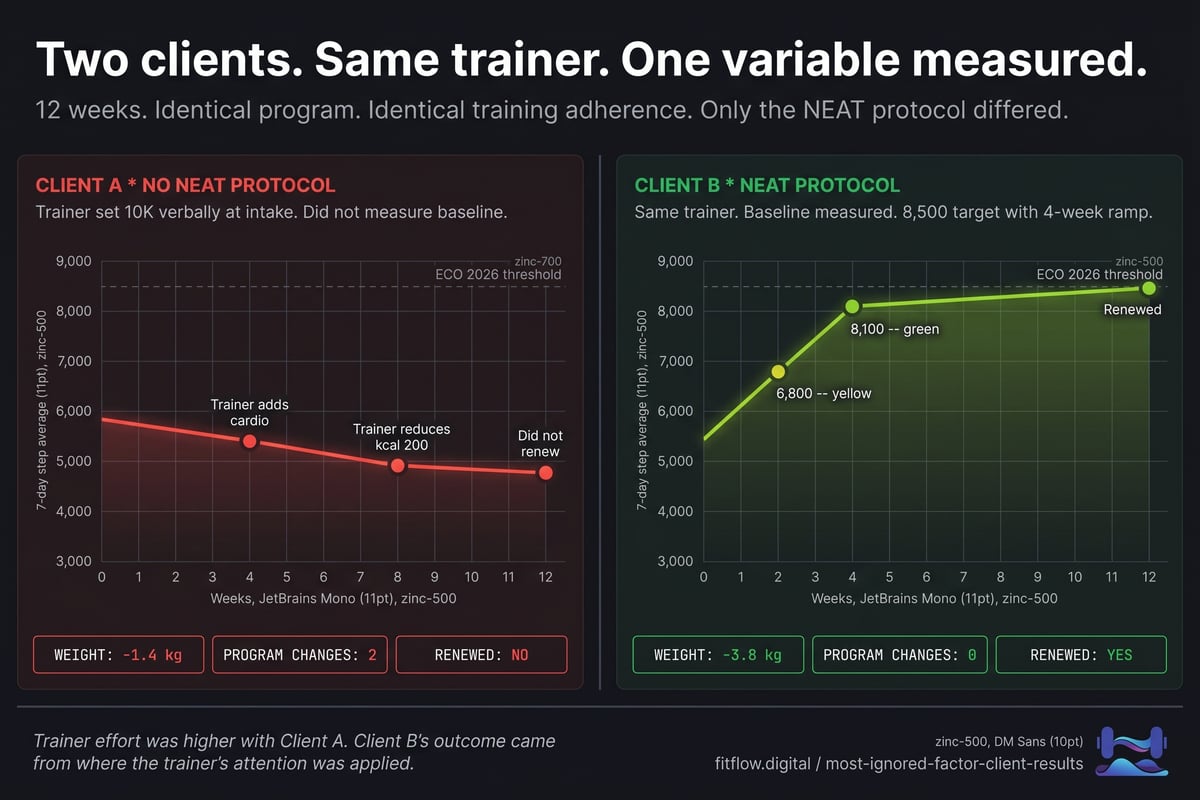
The lesson is not subtle. Program design was identical. Training-session work was identical. The trainer's effort was actually higher with Client A: more programming changes, more caloric adjustments, more troubleshooting time. Client B did better because one number was measured weekly and used before the trainer started rewriting the plan.
The same dynamic is documented in recovery periodization as a programming variable: the input is invisible without measurement, becomes a programming lever once measured, and reorganizes the rest of the system around itself. NEAT is the off-program twin of that pattern.
NEAT and GLP-1 clients
The 2026 trainer reality is that an estimated 8-12% of client books include clients on GLP-1 medications such as semaglutide, tirzepatide, and liraglutide. For these clients, NEAT monitoring is not optional. It is the primary trainer-scope intervention.
The mechanism. GLP-1 medications can push spontaneous activity down. Fatigue at medication initiation, reduced appetite-driven motivation to move, and lower energy availability can all reduce NEAT, often without the client noticing. Multiple 2026 reviews document that fatigue sometimes associated with GLP-1 initiation can reduce NEAT and formal exercise [Cell Reports Medicine, 2026, GLP-1 muscle mass review]. The risk is obvious once you see the stack: rapid weight loss, lower intake, lower daily movement, and a training stimulus that may not be enough to protect lean mass.
The adjusted threshold. Use the GLP-1 row of the threshold table above. The Red Zone trigger is a 25%+ drop in 7-day step average from the pre-medication baseline. That trigger is more sensitive than scale weight for muscle-preservation purposes. By the time the scale shows a problem, the lean-mass loss may already be weeks deep.
The trainer's role, in scope:
Establish the pre-medication step baseline when possible.
Set a NEAT-protection floor (typically 7,000 steps minimum).
Schedule daily structured 10-minute walks as "minimum effective dose" movement scaffolding.
Use the weekly step trend as the primary monitoring metric for muscle-preservation risk.
Out of scope: adjusting medication dose, providing nutritional therapy for medication-induced GI symptoms, or treating clinical-level muscle loss. Those belong to the prescribing provider and a registered dietitian.
The coordination protocol. The trainer should have the client share their step-trend dashboard with their prescribing provider quarterly. That positions the trainer as an early-warning layer for the medical team, not a competitor to it. The posture is simple: "I see the movement data early, and I escalate when the trend turns."
For the full GLP-1 client coaching framework, including dietitian referral criteria and medication-specific protocol adjustments, see the full GLP-1 client coaching framework including referral criteria.
How technology helps at scale
The NEAT diagnostic protocol works well for a trainer with 8-12 clients. At 30-50 clients, manually pulling 7-day step trends from individual phones can eat the whole Monday morning. Without automation, the protocol usually gets dropped within 90 days. This is the scaling boundary a lot of busy trainers hit.
FitFlow is our product. We built the step-trend dashboard because we hit this scaling problem in our own client management. Honest disclosure: this section describes FitFlow's NEAT monitoring features. We are not claiming superiority over Trainerize, TrueCoach, or PT Distinction. We are showing what the protocol looks like when software handles the boring part.
What the dashboard does:
Auto-syncs daily step data from Apple Health, Google Fit, Garmin Connect, Fitbit, and Whoop via OAuth integrations into a client roster view.
Calculates 7-day rolling averages and trend direction (rising / stable / falling) automatically.
Color-codes the roster Green, Yellow, Red against the phase-aligned threshold table each client is assigned to.
Sends trainer alerts when a client crosses from Green to Yellow or Yellow to Red.
Shows the relationship between weekly step trends and the outcome metric: scale, body composition, or performance.
The technology principle: software should automate measurement and surfacing, not the coaching decision. The trainer still makes the call. The dashboard just makes sure the call is informed by data that used to be scattered across 30 client phones and several wearable ecosystems. For the broader walk-through of the integrated client management view, see a complete walk-through of the client management dashboard. For the nuance on what wearable step accuracy can and cannot tell you at the individual level, see wearable step accuracy nuance and interpretation.
The same principle applies whether you build the workflow inside FitFlow or replicate it in your existing stack: automate the measurement, protect the decision.
Scope of practice
Running the NEAT protocol does not turn a personal trainer into a clinician. The professional boundary is clear; staying on the correct side of it is non-negotiable.
In scope (no licensure required):
Set general step targets aligned with client phase.
Educate clients on NEAT and adaptive thermogenesis.
Track and discuss step trends in coaching conversations.
Recommend structured walking as activity scaffolding.
Coordinate with medical providers as the upstream movement-data layer.
Reference the trainer-scope nutrition frameworks: hand portions, plate method, habit-based for the dietary side of the same coaching scope.
Out of scope (requires referral):
Prescribing step counts as treatment for medical conditions, including cardiovascular rehabilitation, post-surgical recovery, and chronic disease management.
Adjusting GLP-1 or other medication-related activity prescriptions.
Treating eating disorders manifesting as compulsive step-counting or exercise compulsion.
Interpreting wearable-derived clinical metrics beyond steps, such as ECG, blood oxygen, or atrial fibrillation alerts.
The professional posture is straightforward. A personal trainer who runs the NEAT protocol is operating within scope. A personal trainer who frames step targets as a prescription for medical weight loss is not. The distinction is structural coaching recommendation versus medical intervention. Stay on the structural side.
Red flag for referral. If a client begins compulsive step-counting, hides activity data, manipulates wearable settings to inflate counts, or expresses guilt or anxiety about missed targets disproportionate to the situation, treat that as a behavioral-health signal. Pause the protocol and refer to a mental health professional with eating-disorder specialization.
Disclaimer. The guidance in this article is general activity coaching within the scope of personal training certification. It does not replace medical advice, prescription-strength activity guidance for clinical populations, or behavioral health treatment for compulsive exercise patterns. Trainers must verify their specific state's regulations regarding scope of practice.
Your 30-day implementation roadmap
Adoption fails when a protocol is introduced as a project. It succeeds when it is folded into the routine that already exists. The roadmap below assumes you already run weekly check-ins; it inserts the NEAT layer into that existing cadence rather than asking you to build a new one.
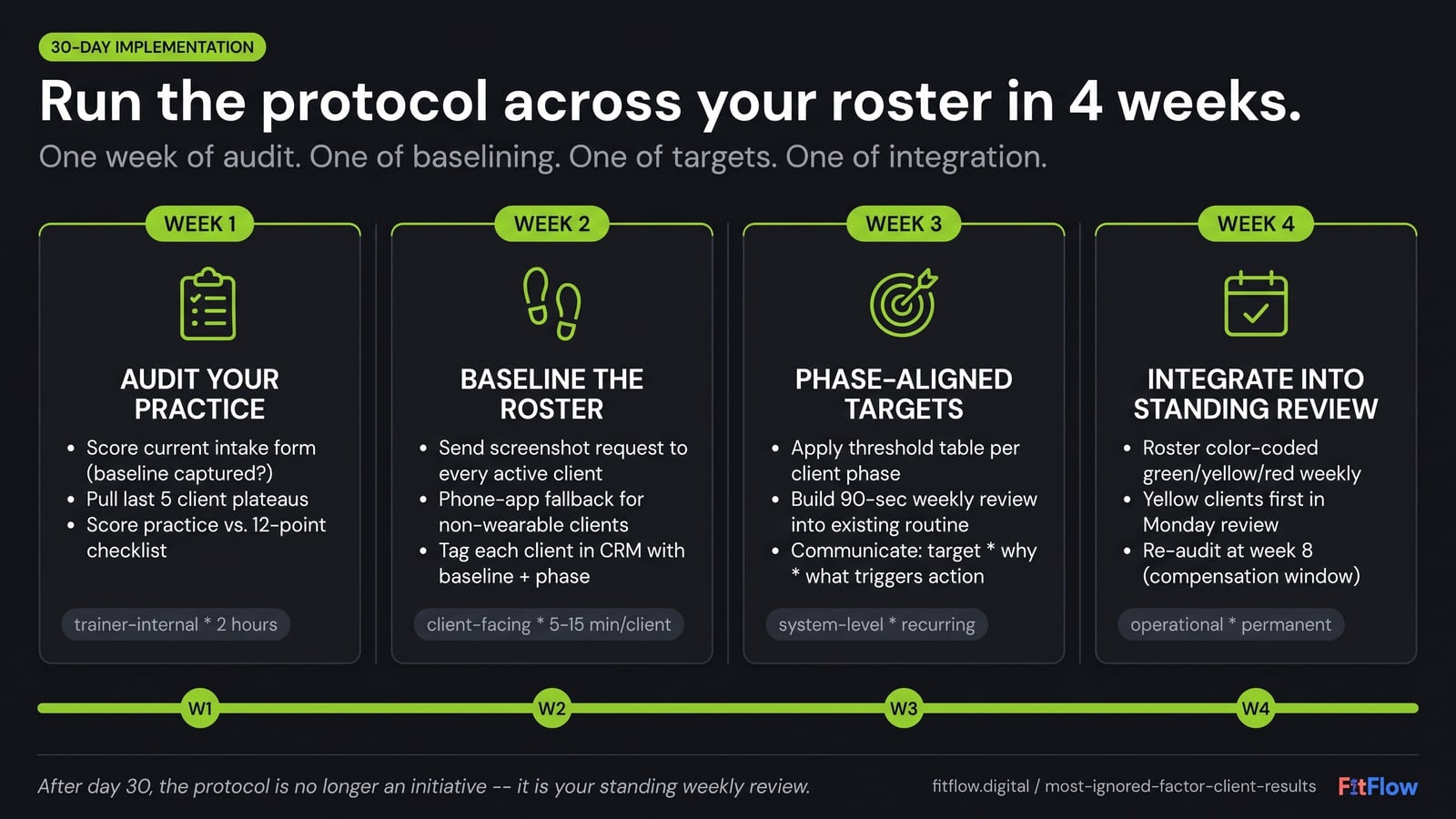
Week 1: audit your current practice.
Score your current intake form. Do you capture a 7-day baseline step count? If not, that is the first failure point.
Pull the last five client plateaus from your records. For each, ask: did I check the step trend before changing the program? If you cannot answer because you did not have the data, your system has the gap.
Download the 12-Point NEAT Diagnostic Checklist and score your own practice.
Week 2: establish baselines across your existing roster.
Send each client a short message: "Hey, can you screenshot your 7-day step trend from your Health app or watch and send it to me? Just for baseline. No judgment."
For clients without wearables, use the phone health-app baseline. The directional accuracy is sufficient.
Tag each client in your CRM or training app with their baseline number and current phase.
Week 3: set phase-aligned targets and the weekly check-in cadence.
Set targets per the threshold table: 8,500 for fat loss; 7,500-8,500 for maintenance; 6,500-8,000 for hypertrophy; phase-specific for performance; 7,000 floor for GLP-1.
Build the weekly check-in into your existing routine. The 90-second step-trend review takes the place of the vague "how was your week" opening question.
Tell clients explicitly: "We are tracking one number every week. Here is the why, here is the target, here is what we will do if it drops."
Week 4: run your first full diagnostic cycle and identify your protocol gaps.
Pull a 7-day average for every client. Color-code per the threshold table.
Identify your Yellow and Red clients. For each, ask: was this client at risk last week and I did not know? Almost always, yes.
For Red clients, intervene with friction-reduction: walking calls, lunchtime walks, structured movement scaffolding. Do that before changing program or calories.
Document the patterns you observe. Prepare to expand the protocol across your full roster.
The 30-day outcome: a working NEAT diagnostic protocol across your client base. Documented baselines. Phase-aligned targets. Weekly trend monitoring. The step trend now sits inside your coaching system instead of being buried in separate client phones.
Key takeaways
NEAT is one of the strongest off-program variables a trainer can track. Inter-individual NEAT range is up to ~2,000 kcal/day [Levine, 1999/2002]. In a deficit, NEAT can drop by 20-40% [Müller et al., 2015; Hall, 2012].
The 2026 operating threshold is about 8,500 steps. ECO 2026 (May 12-15, Istanbul) includes an 18-trial meta-analysis linking that range with better sustained weight-maintenance outcomes [Int J Environ Res Public Health, 2026]. Replace the default "10,000 steps" target with a phase-aligned number.
The data is already on your client's wrist. Wearable technology has been ACSM's #1 fitness trend for 20 consecutive years [ACSM, 2026]. The missing piece is not measurement availability; it is the trainer's protocol for interpreting the number.
Phase-aligned targets beat generic 10K recommendations. Fat loss: 8,500-10,000. Maintenance: 7,500-8,500. Hypertrophy: 6,500-8,000. Strength: 7,000-9,000. GLP-1: protected floor at 7,000.
Trend matters more than absolute. A 7-day rolling average plus trend direction is the diagnostic signal. The Step-Up Trial secondary analysis (Bonomi et al., PMC5970037) shows step pattern, not single peak days, predicts weight-loss success.
For GLP-1 clients, NEAT monitoring is a practical trainer-scope intervention. Medication-related spontaneous-activity decline can accelerate muscle-loss risk [Cell Reports Medicine, 2026].
Run the diagnostic before you change the program. If the step trend has dropped, the bottleneck may be NEAT compensation rather than program design.
One variable. Five measurements. About 90 seconds per week. The protocol is small enough to run and still useful enough to change coaching decisions.
Put the protocol to work today. Download "The Ignored Variable Audit: 12-Point NEAT Diagnostic Checklist for Trainers", the printable scoring tool that runs the 5-measurement protocol in under 15 minutes per client. Get the free checklist ->
Frequently Asked Questions
Comments