The Supplement Reality Check: 5 Worth Taking, 15 You Can Skip
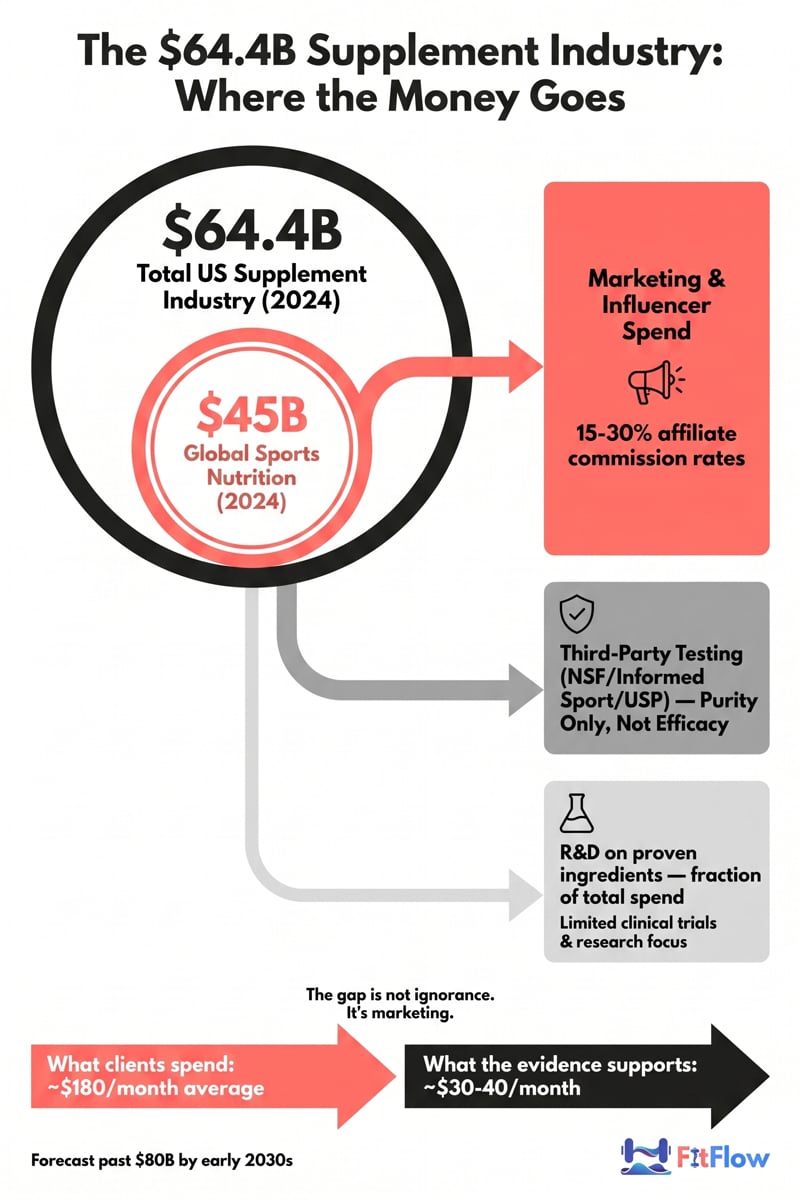
The average fitness client spends roughly $180 a month on supplements. Peer-reviewed evidence supports about $30 of that spend. The gap isn't ignorance. It's a $64.4B persuasion machine [1] aimed directly at your clients' credit cards, and because most trainers stay silent (fearing scope-of-practice lines they don't fully understand), influencer stacks fill the vacuum [2].
This is not a consumer tier list. It is a professional-use guide: the evidence summary and the legal frame you need to have one honest, defensible conversation when a client slides a supplement invoice across the table. We cover the industry economics first, then the legal precedent that should change how every trainer talks about supplements, and only then the actual 5-plus-15 list. By the end you will have a four-question client script you can use this week.
Why Trainers Need to Understand Supplements (Even If They Can't "Prescribe" Them)
The fitness supplement category is one of the largest unregulated consumer markets in the world. The global sports nutrition segment was valued at approximately $45B in 2024, with broader supplement industry estimates exceeding $64B and forecasts pointing past $80B by the early 2030s [1][3]. Marketing spend per dollar of revenue here exceeds the ratio seen in most pharmaceutical categories. Affiliate commissions on supplement sales commonly run 15–30% [4], which means a meaningful share of "evidence-based" fitness creators online are paid percentages on the same products they review.
Your clients do not see any of this. They see a confident person on a screen who already has the body they want, holding a tub of something. When they ask what you think, you have three options. You can say "I don't recommend supplements" (true, defensible, useless). You can endorse the product (commercially appealing, legally dangerous, often dishonest). Or you can do what registered dietitians do with their non-RD referrals: translate the evidence in plain language and stay on your side of the scope line.
This third option is the only one that builds trust and protects your practice. It is also the only one that distinguishes you from a vending machine.
Sidebar: Scope of Practice and the Capati Case
In 1998, Anne Marie Capati, a Crunch Fitness client in her 30s with diagnosed hypertension, collapsed at the gym and died of a brain hemorrhage 14 hours later. Her personal trainer had recommended several dietary supplements, including ephedra-containing products. The case (Capati v. Crunch Fitness International, Inc., 295 A.D.2d 181, 743 N.Y.S.2d 474, N.Y. App. Div. 2002) ultimately settled for more than $4M in 2004 and remains the defining legal precedent for trainer supplement liability in the United States [5].
The boundary is straightforward in principle and fuzzy in practice. As a personal trainer without an additional RD, RDN, or licensed clinical credential, you can share general, publicly available nutrition information [6]. You cannot diagnose deficiencies, prescribe therapeutic doses, or recommend supplements to treat medical conditions. Scope rules vary by state and by certifying body, so confirm your specific guidance with NFPT, NASM, ACE, or your liability insurer [6][7].
The practical implication: the safest sentence you will ever say to a client about supplements is some version of "Here is what the published research shows for the general population. For your specific situation, a registered dietitian or your physician is the right resource." That sentence is defensible. "You should take X" is not.
The 5 Supplements With Actual Evidence Behind Them
These five are boring, inexpensive, and unglamorous — which is exactly why the supplement industry would rather talk about anything else. The combined monthly cost is roughly $30–$40. Everything beyond it is, charitably, optional.
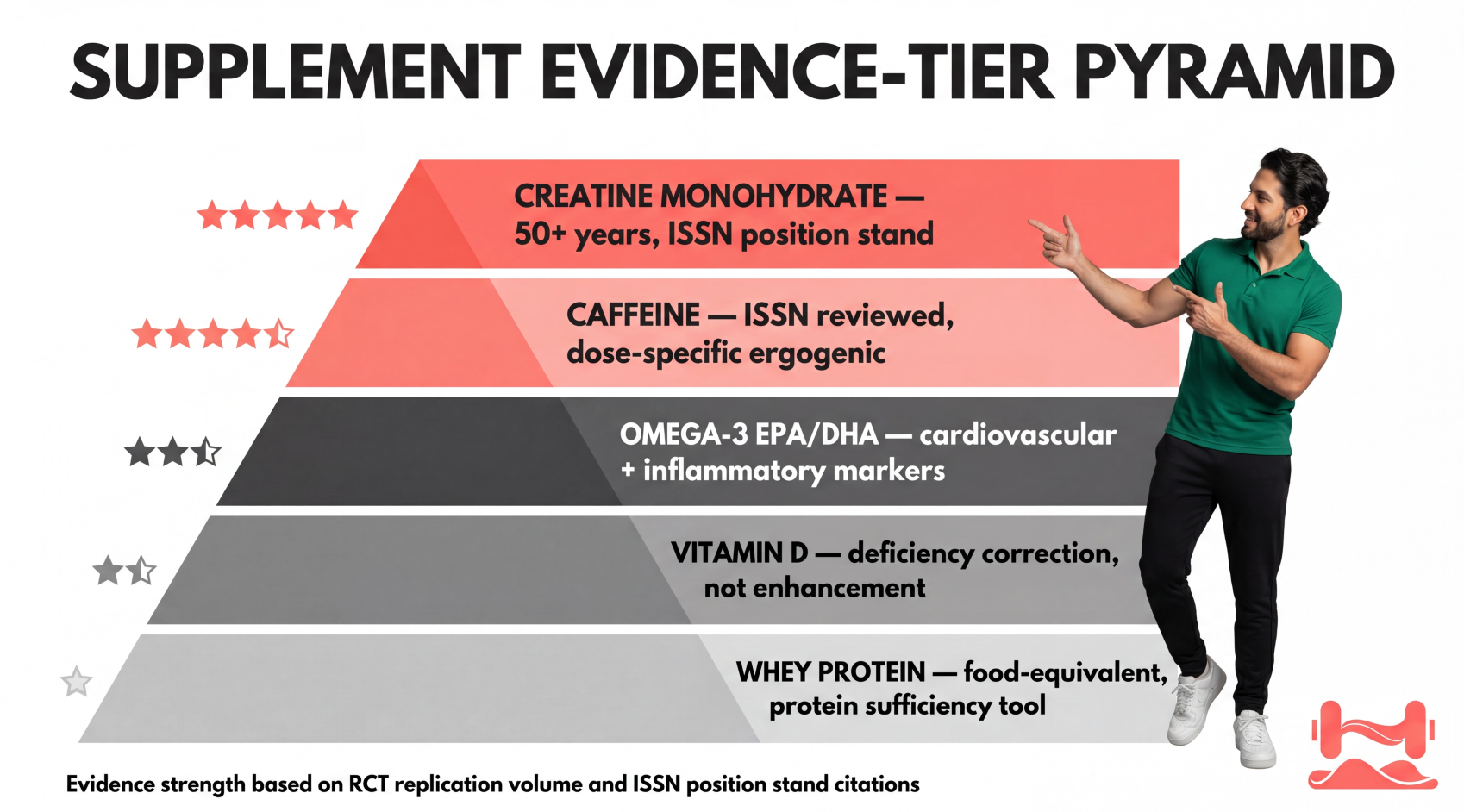
1. Creatine Monohydrate (3–5g/day)
The International Society of Sports Nutrition (ISSN) position stand describes creatine monohydrate as the most effective ergogenic nutritional supplement available to athletes for increasing high-intensity exercise capacity and lean body mass [8]. Supplementation up to 30g/day for five years has been demonstrated safe and well-tolerated in healthy individuals.
Mechanism: phosphocreatine replenishment supports rapid ATP regeneration for high-intensity work, with emerging evidence for cellular hydration and neural energetics.
Dose: 3–5g/day, indefinitely. A loading phase (20g/day for 5–7 days) accelerates saturation but is optional. Creatine HCl, buffered creatine, and other "advanced" forms are not meaningfully superior to monohydrate despite higher prices [8].
Trending angle — women and menopause: The 2026 CONCRET-MENOPA randomized trial added to a growing body of work suggesting benefits for lean mass preservation, bone health, and cognitive function in peri- and post-menopausal women [9]. The signal is real, but coverage has at times outrun the evidence. Recent journalism correctly cautioned that broader claims (mood, brain protection) remain preliminary [10]. The defensible framing: lean-mass and strength evidence is strong for women across the lifespan; secondary claims should be tracked, not parroted.
Cost: ~$15–20/month. Trainer framing: "This is the one supplement where I won't hedge. The evidence is fifty years deep."
2. Whey Protein (As Food, Not Magic)
Whey is not a supplement in the pharmacological sense. It is a concentrated food — chicken in a bag. The question is not whether whey works, but whether your client needs it to hit total daily protein targets from whole food.
A 2025 network meta-analysis of 78 studies (n=4,755) found whey produces a small but statistically significant improvement in both fat-free mass and strength in resistance-trained adults (SMD 0.16 and 0.15) [11]. That same analysis ranked collagen first on fat-free mass, a finding the authors flag as preliminary given fewer underlying trials. Across the broader literature, the magnitude of effect depends almost entirely on total daily protein intake. The ISSN protein position stand puts the working target at 1.6–2.2g/kg body weight per day for hypertrophy [12].
Who needs it: clients who cannot realistically hit protein targets from whole food (travel, schedule, appetite, busy parents). Who doesn't: clients already meeting 1.6–2.2 g/kg from whole food. Adding whey beyond targets produces no additional MPS signal, just additional calories.
For translating protein math into something clients actually do, see our simple nutrition frameworks for training clients.
Trainer framing: "Treat whey like chicken in a bag. It's food that happens to come in powder form."
3. Vitamin D (1,000–4,000 IU/day, deficiency-context only)
Vitamin D is on this list because deficiency is unusually common and the performance consequences are non-trivial, not because supplementation is a performance booster in sufficient individuals.
NIH Office of Dietary Supplements data and large population surveys put adult vitamin D inadequacy at roughly 35–40% of US adults, with substantially higher rates in northern latitudes, darker-skinned individuals, indoor workers, and people avoiding sun exposure [13]. Deficiency correlates with reduced muscle function, slower recovery, increased injury risk, and impaired immune response.
Dose: 1,000–4,000 IU/day is the NIH/ODS-supported range for adult deficiency correction without serum testing. The gold standard is a 25-OH-D blood test before high-dose supplementation, and that test sits firmly outside trainer scope. Refer to a physician for testing and any dose above 4,000 IU/day.
Cost: ~$5–10/month. Trainer framing: "This one is about correcting a drag, not adding a superpower. If your client works indoors through winter, the odds say they're deficient."
4. Omega-3 Fatty Acids — EPA/DHA (1–3g combined/day)
EPA and DHA, the long-chain omega-3s in fatty fish and algal oil, reduce pro-inflammatory cytokines and support cardiovascular and joint health [14]. The performance evidence is meaningful for clients with low fish intake, modest for clients who already eat fatty fish twice weekly.
Important distinction: EPA/DHA from fish oil or algal oil is the evidence-supported form. ALA (alpha-linolenic acid from flaxseed and chia) converts to EPA/DHA inefficiently in humans (~5–15%). Algal oil is the evidence-equivalent vegan option.
Dose: 1–3g combined EPA + DHA per day. Read the label: many "1,000mg fish oil" capsules contain only 200–300mg of actual EPA + DHA.
Cost: ~$15–25/month. Trainer framing: "If your client eats fatty fish twice a week, they can skip this. Most clients don't."
5. Caffeine (3–6mg/kg, timing matters more than dose)
ISSN reviews and large meta-analyses consistently document caffeine improvements in endurance, maximal strength, power output, and perceived exertion at 3–6mg/kg body weight, with effects appearing 30–60 minutes post-ingestion [15].
The problem your clients have is not caffeine. It is timing. Peak plasma concentration occurs around 60 minutes post-dose, and caffeine's half-life is 5–6 hours in most adults. A 400mg pre-workout at 6pm still has roughly 200mg circulating at midnight, enough to compress slow-wave sleep architecture and degrade recovery in caffeine-sensitive individuals.
For more on protecting sleep as the primary recovery variable, see our breakdown of recovery as a growth lever.
Dose: 3–6mg/kg pre-training (200–400mg for most clients). Tolerance develops within 1–2 weeks of daily use; cycling (5 days on, 2 days off) or strategic abstinence (4–7 days before a key event) restores full ergogenic response.
Trainer framing: "Caffeine works. The problem is your clients taking 400mg pre-workouts at 6pm and wondering why they can't recover."
Want to give clients a one-page evidence summary instead of forwarding this article? Download The Trainer's Supplement Quick-Reference Card — all 20 supplements covered here, on a single printable page, with evidence tier, dose range, and scope-of-practice talking points. Free for FitFlow members.
The 15 Supplements to Skip (Organized by Failure Mode)
Grouped by why they fail, because the failure category is more useful than a flat "don't buy this" list. Knowing the failure mode lets you give a better answer than "the research is mixed."
Category 1 — Redundant If Protein Is Adequate
6. BCAAs. Muscle protein synthesis requires all nine essential amino acids. Isolated BCAAs produce roughly half the MPS response of an equivalent dose of whey because the other six EAAs are rate-limiting [12][16]. The only narrow evidence-based use case is fasted training, and even there a small amount of whey accomplishes the same thing at lower cost. Cost waste: $30–50/month.
7. Glutamine (standalone). Marketed for immune function and gut health; in well-nourished exercisers, evidence is not meaningful. The clinical use cases (severe burns, critical illness) do not transfer to healthy gym populations [17].
8. Non-BCAA EAA blends layered on top of adequate protein. Same redundancy as BCAAs. Whole protein sources deliver all EAAs plus micronutrients and satiation at lower cost per usable gram.
Category 2 — Ingredient Works, Product Is the Problem
9. Pre-Workout Blends (MIPS). Caffeine works. Beta-alanine works at 3.2–6.4 g/day chronically. Nitrates work. The blend is the problem: MIPS contain 10–30 ingredients, frequently in proprietary blends that obscure individual doses. A JISSN safety review classified MIPS as high-risk dietary supplements due to inadequate safety data on the combinations used [18]. Buy the proven ingredients separately.
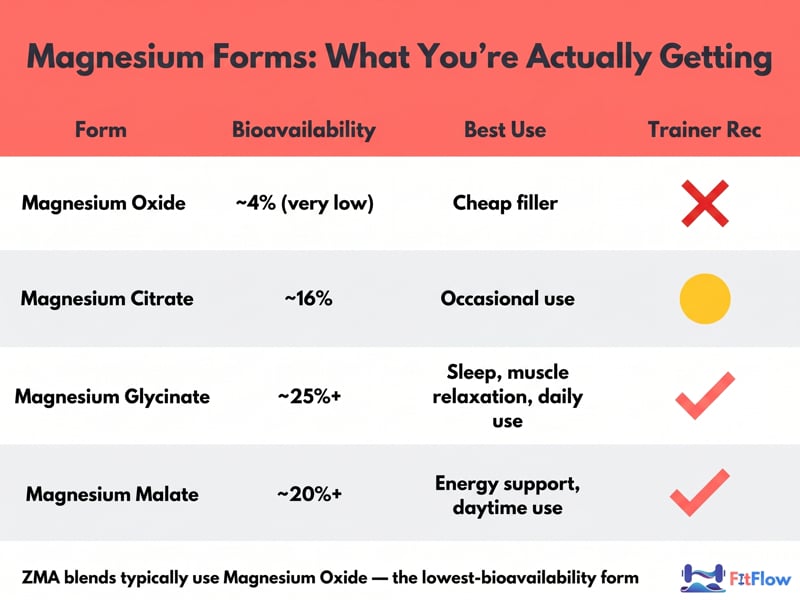
10. ZMA (Zinc-Magnesium-B6). ZMA blends typically use magnesium oxide (~4% bioavailability) and underdose both minerals relative to research protocols [19]. The better choice when magnesium is indicated: magnesium glycinate or magnesium malate at 200–400mg before bed (well-absorbed, no laxative effect, reasonable sleep-quality evidence in deficient populations) [19].
11. Greens Powders. Do not replicate the fiber matrix, water content, or thousands of bioactives in whole produce. The European Food Safety Authority has not authorized health claims for the majority of greens powder ingredient classes [20]. Reframe: "If your budget includes $60/month for greens powder, your budget includes more vegetables."
Category 3 — No Meaningful Evidence of Effect
12. Testosterone Boosters. A peer-reviewed analysis found ~90% of T-booster product label claims had no supporting clinical data; only 24.8% of products contained any ingredient with replicated evidence of raising endogenous testosterone in healthy adult men [21]. D-aspartic acid shows null or negative effects in well-controlled trials. The FDA has flagged multiple products in this category for undisclosed pharmaceutical contamination.
13. Tribulus Terrestris. Decades of human trials in resistance-trained men show no consistent increase in testosterone, lean mass, or strength beyond placebo [21]. Persists in proprietary blends.
14. Fat Burners / Thermogenics. Ephedra was removed from the US market in 2004 after deaths including the Capati case [5]. Remaining legal thermogenics (synephrine, yohimbine, capsaicin) show modest effects at best with cardiovascular risk in susceptible individuals. None has demonstrated clinically meaningful fat loss independent of caloric deficit.
15. Raspberry Ketones. Animal data at very high doses, no credible human evidence [22]. Popularized by daytime television.
16. Garcinia Cambogia. Multiple randomized human trials show no meaningful difference vs. placebo for weight or fat loss [22]. Hepatotoxicity case reports exist.
17. Deer Antler Velvet (IGF-1 spray). Banned by WADA, has never demonstrated meaningful IGF-1 elevation or performance benefit at consumer doses.
18. Generic "Adaptogen" Stacks. Ashwagandha has reasonable evidence for cortisol and perceived-stress reduction in stressed populations; rhodiola has mixed evidence for fatigue [23]. The generic adaptogen stack, a proprietary blend marketed as a "natural test booster" or "cortisol blocker," typically underdoses each ingredient. Redirect clients to sleep, training load, and total nutrition, which actually move those markers.
Category 4 — Narrow Application, Overhyped Beyond It
19. Collagen Supplements (for muscle building). Ingested collagen is digested to amino acids (predominantly glycine and proline, both non-essential) before absorption [24]. A 2025 network meta-analysis surprised many by ranking collagen first for fat-free mass gain in resistance training, but the authors caution the result rests on fewer underlying trials and shorter durations than the whey evidence base and needs replication [11]. There is a narrow connective-tissue use case (vitamin-C-plus-collagen pre-exercise, one small trial). For now, collagen-for-muscle is an emerging-evidence call, not a confident recommendation, and should not displace a complete protein source.
20. HMB in trained populations. In untrained novices and clinical wasting, HMB has some evidence. In resistance-trained adults, the population most likely to buy it, Sanchez-Martinez et al.'s 2018 meta-analysis in the Journal of Science and Medicine in Sport found no significant effect on strength or body composition [25]. Skip for trained clients.
Category 5 — Timing and Form Mismatch
21. CLA (Conjugated Linoleic Acid). Human trials are inconsistent; effects where they appear are small and not clinically meaningful compared to a basic caloric deficit [22].
22. High-Dose Antioxidants (vitamin C >1,000mg or vitamin E >400 IU around training). The counter-intuitive finding most trainers haven't heard: pharmacological doses of antioxidant vitamins around training may blunt the reactive oxygen species (ROS) signaling that drives mitochondrial biogenesis and strength adaptations. That blunts the very adaptations your client is training for [26]. Food-sourced antioxidants do not carry this risk.
23. High-Dose Melatonin (5–10mg). Melatonin is a neurohormone, not a sedative. In the landmark Zhdanova et al. dose-response trial (JCEM 2001), a physiological 0.3mg dose restored sleep efficiency in older adults as effectively as 3.0mg; the larger dose produced supraphysiological plasma levels without additional benefit [27]. The evidence-supported range is 0.3–1mg taken 30–60 minutes before lights-out. Most US products contain 5–10mg, which is 5–30x higher than necessary. Trainer framing: "The dose on the bottle is probably ten times the evidence-supported dose. Cut the tablet."

The Industry Economics Your Clients Don't See
The reason this list looks the way it does is structural, not accidental:
Market size: Global supplement industry ~$64.4B in 2024; sports nutrition ~$45B [1][3]. Projections through 2030 put it past $80B.
Marketing-to-revenue ratio: Supplement marketing spend per dollar of revenue exceeds pharmaceutical industry norms in many sub-categories. The business model depends on persuasion, not pharmacology.
Affiliate economics: A meaningful share of "evidence-based" fitness creators earn 15–30% commission on supplement sales [4]. The same person reviewing a product on a podcast is often the affiliate selling it. Not illegal. Not always disclosed clearly. Something your clients should know.
Third-party testing gap: NSF Certified for Sport, Informed Sport, and USP certifications verify purity, not efficacy. A product can pass NSF testing and have zero published evidence of benefit.
The certification logo means the product is what it says it is, not that what it says it is actually works.
Sidebar: The Affiliate-Income Trade-Off
If you have been running a supplement affiliate stream as a side revenue source, run the math honestly. Industry surveys put typical fitness affiliate income for trainers with mid-sized followings at a few hundred to a few thousand dollars per month, with most under $1,000/month and a small minority over $5,000 [4]. Compare against client retention: one additional retained client at $400/month for twelve months is $4,800 in revenue you keep entirely. If your affiliate stream costs you even one client of trust per year, you are net negative. The trainers winning long-term are quietly shifting toward platform fees, group programming, and education products they own.
Sidebar: turn this article into a client conversation tool. The Trainer's Supplement Quick-Reference Card is the one-page printable companion — designed to keep on your clipboard during check-ins. Get it free.
Scope of Practice: What You Can and Cannot Say
The principle in one sentence: you can share general, publicly available evidence summaries; you cannot diagnose, prescribe, or treat [6][7].
You can say: "Research suggests creatine monohydrate at 3–5 grams per day is safe and well-studied for general training populations. Whether it makes sense for you specifically is a conversation for your physician or a registered dietitian."
You cannot say: "You should take 5 grams of creatine per day to fix your low energy" (prescribing, diagnosing).
Red flags requiring referral, not opinion:
Client presenting a supplement for a specific health condition (thyroid, hormone, chronic illness, mental health)
Client stack with eight or more products
Client on prescription medications (especially anticoagulants, antidepressants, cardiovascular drugs)
Client pregnant, postpartum, or breastfeeding
Document the conversation. Note in the client file: date, what was discussed, what referral recommendation you made. Trainers deposed in supplement-adjacent cases consistently lose ground without contemporaneous documentation.
The deeper liability asymmetry: being vague and unhelpful carries no legal exposure. Being specific and wrong does.
For broader context on the off-program variables that drive client outcomes more than supplements ever will, see how to improve results without changing training and why your clients are not recovering.
The Four-Question Framework for Any Supplement Conversation
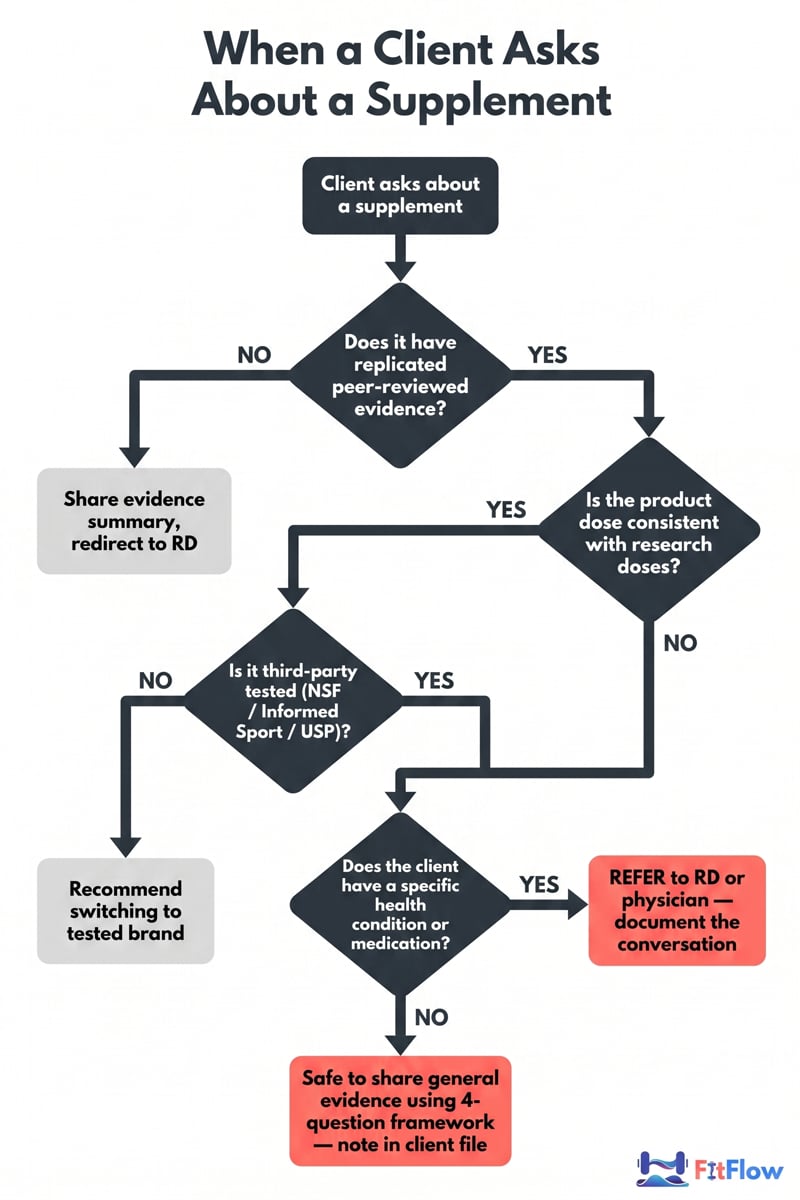
When a client asks about a supplement, walk through these out loud. The framework gives you a defensible structure and turns the conversation into evidence translation instead of opinion.
Is there replicated, peer-reviewed evidence for the claimed benefit? Not one study. A body of evidence, ideally including a systematic review or meta-analysis.
Is the dose in this product consistent with the doses used in the research? Most consumer products are underdosed (proprietary blends) or overdosed (melatonin).
Is this product third-party tested for purity? NSF Certified for Sport, Informed Sport, or USP. Required for any client subject to drug testing; recommended for everyone else.
Does this specific client have a reason to think they're deficient or would benefit beyond baseline? Deficiency context changes the calculus for vitamin D, omega-3, and magnesium.
If a supplement fails any one of these four, the answer is "the evidence doesn't support it for you right now." If it passes all four, the answer is "the research supports it; talk to your physician or dietitian about whether it fits your situation."
That is the entire script. You can keep it on a card.
Key Takeaways
The 5 worth taking: creatine monohydrate (3–5g/day), whey protein (as food, only if needed to hit targets), vitamin D (1,000–4,000 IU/day when deficient), omega-3 EPA/DHA (1–3g combined when fish intake is low), caffeine (3–6mg/kg pre-training, timed to protect sleep). Total: ~$30–40/month.
The 15 to skip group into five failure modes: redundant given adequate protein; ingredient-works-product-doesn't; no meaningful evidence; narrow-but-overhyped; and timing/form mismatch.
Industry economics: A $64B market with pharma-exceeding marketing ratios, 15–30% affiliate commissions, and a third-party-testing system that certifies purity but not efficacy.
Legal precedent: Capati v. Crunch Fitness (settled >$4M, 2004) is the case every trainer should know.
The four-question framework is the entire trainer script: evidence, dose, third-party testing, deficiency context.
Download The Trainer's Supplement Quick-Reference Card — all 20 supplements above, on a single printable page, with evidence tier, dose range, and scope-of-practice talking points. Free for FitFlow members. Pair it with our evidence-based nutrition and recovery guide and the playbook on why perfect diets fail to build a complete nutrition conversation system inside your practice.
Frequently Asked Questions
Comments