Recovery as a Growth Lever: How Sleep, Nutrition, and Stress Periodization Accelerate Adaptation
You wrote the program. You selected the exercises. You periodized the volume, structured the intensification, scheduled the deload. Your client trained consistently for twelve weeks and made good progress for eight. Then something shifted -- not the program, not the effort -- and the results slowed in a way you could not fully explain by looking at the training log.
The program was only ever half the equation. What happened in the 163 hours per week your client was not in the gym determined whether the training produced adaptation or accumulated fatigue. And unlike the training hours, those 163 were probably not planned. Recovery for personal training clients has remained the least structured variable in most programming models -- not because trainers doubt its importance, but because no one built the practitioner framework to plan it.
Recovery is not the absence of training. It is the other half of the adaptation signal. Sleep architecture, nutrition timing, and stress load management are not lifestyle recommendations that sit alongside the training plan -- they are programmable variables that belong inside it. Trainers who periodize recovery alongside training produce measurably faster adaptation than trainers who manage it reactively. The ACSM 2026 Trends Report confirms this shift: wearable technology is the number one fitness trend, and 70 percent of wearable users are now applying biometric data to recovery decisions. The data infrastructure exists. What has been missing is the decision framework.
This is not a new idea in elite sport -- recovery periodization is standard practice in Olympic programming. It has not crossed into general population personal training because no one has built the practitioner framework. This article does. If you learned recovery management as "remind clients to sleep enough and eat enough protein," you learned a useful baseline -- and nobody mentioned it was just the floor.
We built the Recovery-Training Integration Template -- a phase-matched planning tool for sleep, nutrition timing, and stress management alongside your mesocycle structure. Download it free below.
Recovery Is Not Rest. It Is the Other Half of the Adaptation Signal.
Most training plans treat recovery as the negative space between sessions -- the absence of training rather than its complement. That model has a direct corollary in how programs are structured: the plan specifies what the client does during the five training hours per week and is silent about the remaining 163. Recovery for personal training clients remains incomplete by construction when those 163 hours are also variable, also respond to planning, and also determine adaptation outcomes -- yet receive no structure.
Recovery periodization corrects this asymmetry. It treats sleep architecture, nutrition timing, stress load management, and deload design as co-variables inside the training plan, adjusted by mesocycle phase, monitored with the same rigor as volume and intensity.
What Adaptation Actually Requires
Adaptation does not occur during training. It occurs during recovery -- specifically, during the sleep-dependent growth hormone cascade and the 24-48 hour post-exercise protein synthesis window. Training provides the signal; recovery determines whether the signal is answered.
Training creates a stimulus -- mechanical tension, metabolic stress, muscle damage -- that signals the body to adapt. The adaptation itself happens during recovery: when growth hormone is released during NREM sleep, when muscle protein synthesis peaks in the 24-48 hours post-stimulus, when cortisol normalizes and testosterone and IGF-1 return to baseline. If recovery is inadequate, the signal is received but the adaptation is suppressed.
The most recently mapped mechanism makes this dependency concrete. Researchers at UC Berkeley identified the neuroendocrine circuit governing sleep-dependent growth hormone release: GHRH neurons in the hypothalamus trigger the primary GH pulse during the first two to three hours of NREM sleep, modulated by somatostatin inhibition and locus coeruleus feedback UC Berkeley / Cell, 2025. This pulse drives tissue repair, fat metabolism, and protein synthesis. It does not occur on a fixed schedule -- it depends on sleep architecture. A client sleeping seven hours with fragmented NREM and elevated cortisol from chronic stress may receive a fraction of the GH pulse a client sleeping six and a half hours with intact sleep architecture receives.
The downstream consequences are measurable. Lamon et al., 2021 demonstrated that one night of acute sleep deprivation reduces muscle protein synthesis by 18 percent, increases cortisol by 21 percent, and reduces testosterone by 24 percent. The training session you designed for that morning is running on a substrate you did not control.
For the complete evidence base on sleep architecture, protein timing, and supplementation -- see our evidence-based recovery science guide.
The 163-Hour Problem
A typical personal training client trains four to five hours per week. You plan those hours in detail -- exercise selection, volume, intensity, rest intervals, RPE targets, progression logic. The remaining 163 hours per week receive a general recommendation ("get seven to eight hours of sleep, eat enough protein, manage your stress") and no planning.
The asymmetry exists because the training hours are tractable. They happen in a controlled environment with observable outcomes. The 163 recovery hours happen outside your field of view, involve variables the client has not been taught to manage proactively, and are affected by life circumstances -- work, stress, family, social obligations -- that most trainers have historically treated as outside the scope of the training plan.
The consequence is predictable: when clients plateau, trainers adjust the training plan. They change the exercise selection, add volume, modify periodization. Some of these adjustments work. Many do not -- because the plateau is a recovery signal, not a training signal. The training plan was already adequate; the recovery plan was missing. Before periodizing recovery, ensure the five hidden recovery barriers are not actively degrading your client's adaptation capacity -- our diagnostic framework covers the most common ones.
Just as progressive overload has more dimensions than most trainers apply, recovery has more programmable variables than most trainers plan. Both arguments converge on the same principle: multi-dimensional programming is more effective than single-variable management.
The 163 hours are not outside the scope of the training plan. They are half the training plan. And they can be periodized.
The NASM 2026 Top Fitness Trends report stated it directly: "Sleep optimization, stress regulation, and intentional deloads move from optional to expected in periodization." Men's Journal confirmed practitioner demand in March 2026: "Recovery periodization is the key to preventing injury and hitting PRs by adjusting rest to your training and life stress." The concept has arrived. What follows is the practitioner tool.
The 4 Programmable Recovery Variables

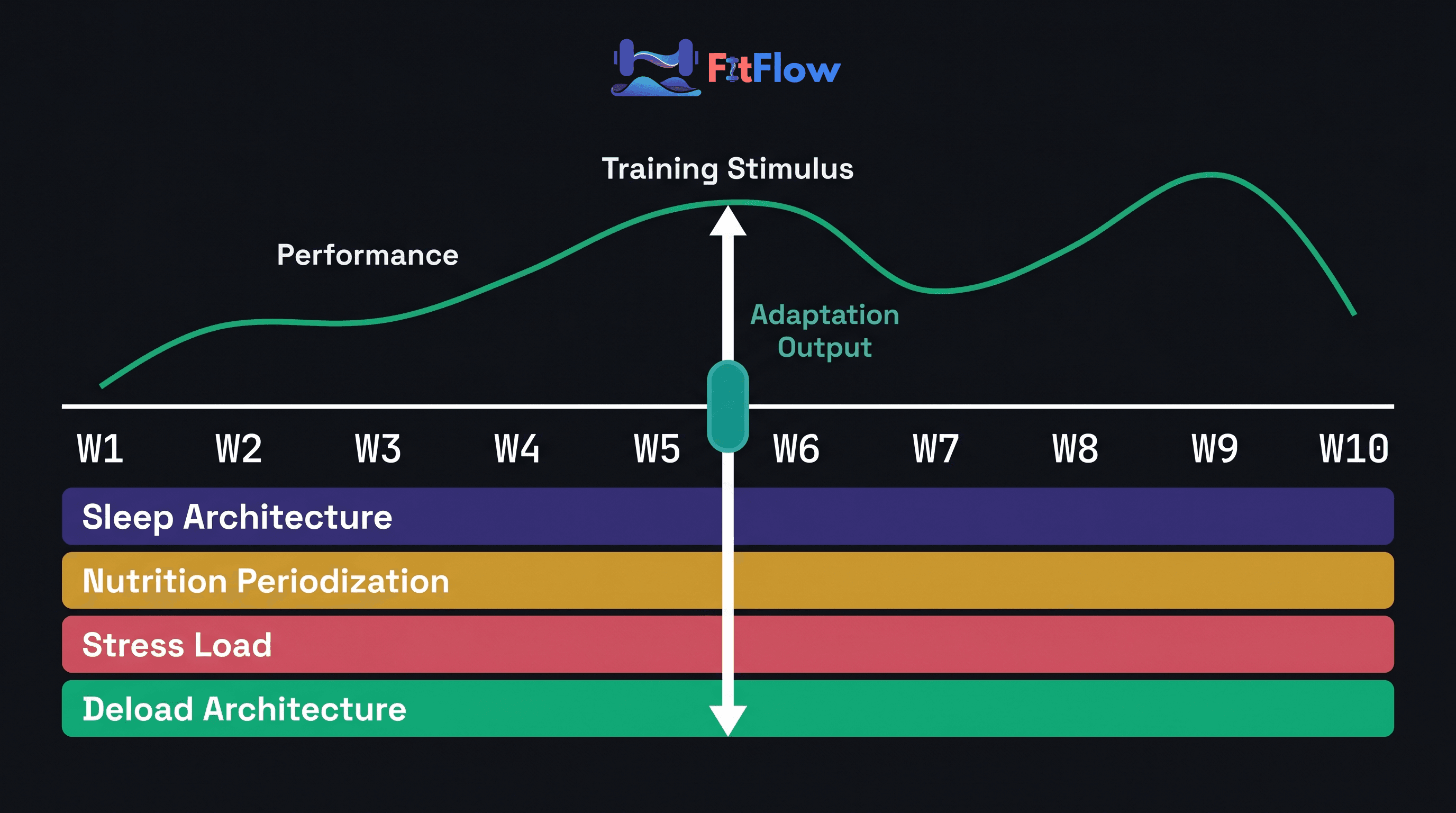
Recovery has four programmable variables. Sleep architecture is the primary driver of GH-mediated tissue repair and hormonal recovery. Nutrition periodization determines the substrate availability for protein synthesis and glycogen resynthesis at each training phase. Stress load management tracks the allostatic load -- the total physiological cost of all stressors, training and non-training -- that determines how much adaptation capacity remains after accounting for life. Deload architecture is the deliberate reduction of training load that allows the other three variables to complete their work without accumulating residual fatigue.
Each variable has a mechanism, phase-specific targets, and a practical signal that changes by mesocycle phase. Here is what you need to know to program each one.
Sleep Architecture
Sleep architecture is not sleep duration. It is the sequential cycling through NREM stages one through three and REM sleep, typically in 90-minute cycles, with the first two cycles being NREM-dominant -- producing the highest growth hormone release -- and the final cycles being REM-dominant.
The mechanism is now mapped at the circuit level. The UC Berkeley/Cell 2025 finding UC Berkeley / Cell, 2025 established that during early NREM (stages two and three, slow-wave sleep), GHRH activity rises and somatostatin inhibition drops, triggering the largest GH pulse of the night. This pulse is time-locked to the first two to three hours after sleep onset -- not to total sleep duration. Disrupting early NREM through late sleep onset, alcohol, or high cortisol suppresses the primary GH pulse regardless of whether the client eventually logs seven hours.
Dattilo et al., 2011 demonstrated that sleep debt increases protein breakdown pathways and inhibits protein synthesis, favoring muscle atrophy. Vitale et al., 2019 confirmed the multi-dimensional relationship: sleep stage specificity matters more than total sleep duration for athletic recovery outcomes. Frontiers in Sports and Active Living, 2026 reinforced that optimizing sleep architecture is among the most effective recovery strategies for performance.
Phase-specific targets for your clients:
Accumulation phase (high volume, building stress): Sleep demand is highest. Target 7.5 to 9 hours with sleep onset before midnight and no alcohol within three hours of sleep. The adaptation signal from high-volume weeks is GH-dependent; shortchanging NREM suppresses the return.
Intensification phase (high intensity, moderate volume): Sleep duration can normalize at seven to eight hours if architecture quality is maintained. Pre-sleep cortisol management -- no high-stress tasks in the final hour before bed -- is the priority variable.
Realization phase (peak performance, tapered volume): Sleep duration is not the limiting factor. Consistency of sleep schedule -- wake time within 30 minutes of the daily target -- drives circadian entrainment and predictable GH timing.
Deload phase: Sleep is the primary recovery driver. Increase to eight to nine hours if possible. This is when accumulated adaptation from the previous block is consolidated.
For a complete review of sleep architecture research -- see our Evidence-Based Nutrition and Recovery Guide.
Practical signal: Ask about sleep onset time and perceived sleep quality -- not just duration. A client sleeping eight hours starting at 1:00 am has a different GH profile than the same client sleeping eight hours starting at 10:30 pm.
Nutrition Periodization
Sleep architecture governs hormone release. The next variable governs what those hormones have to work with.
Nutrition periodization in this context is the strategic adjustment of nutrient timing, macronutrient distribution, and total energy availability across mesocycle phases to match the recovery demands of each phase. This is not carb cycling and it is not the sports nutrition periodization framework designed for competitive athletes. It is the practitioner tool for general population clients in a structured training block.
Three timing windows change by phase:
Pre-workout fueling adjusts by phase. During accumulation (high volume), pre-workout carbohydrate becomes more critical for sustained session quality -- sessions are longer, more glycolytic. During intensification (high intensity), pre-workout focus shifts toward readiness: a lighter, earlier meal to minimize gastrointestinal stress under heavy loads. During deload, pre-workout fueling can normalize to the client's baseline preference.
Post-workout protein timing remains consistent across phases (30-to-60-minute window, 20 to 40 grams of protein) but the type and accompanying carbohydrate shifts. During accumulation, co-ingestion of carbohydrate with post-workout protein speeds glycogen resynthesis for back-to-back high-volume sessions. During realization, faster-digesting protein sources optimize muscle protein synthesis for peak performance blocks. The strategic manipulation of macronutrients across mesocycle phases is well established in the periodized nutrition literature Jeukendrup, 2017, and recent work by Morton et al., 2025 confirmed that nutritional periodization strategies enhance both training adaptation and recovery in applied settings.
Between-session fueling is the most commonly neglected variable. During high-volume accumulation phases, total energy availability must remain above the MPS threshold -- approximately 0.4 to 0.55 grams of protein per kilogram per meal across four meals minimum. Under-fueling between sessions is a common pattern when clients conflate "training for results" with "eating less." It suppresses MPS and converts the training stimulus from anabolic to catabolic.
For practical nutrition compliance frameworks -- see Simple Nutrition Frameworks That Actually Work.
Practical signal: Nutrition periodization for recovery does not require precise macro-tracking for general population clients. It requires three decisions per phase: pre-workout strategy, post-workout strategy, and between-session fueling floor.
Stress Load Management
Allostatic load is the cumulative physiological cost of all stressors -- training and non-training. The body does not distinguish between work deadlines, relationship strain, commuting, and sets of Romanian deadlifts. All generate cortisol. All draw from the same recovery capacity pool.
Think of it as an adaptation budget: every client has a finite weekly adaptation budget determined by their recovery capacity -- sleep quality, nutrition adequacy, baseline health. Training draws from that budget deliberately. Life stress draws from the same budget without consent. When life stress consumes a large share of the budget, the adaptation return on the training stimulus drops. Kellmann et al., 2018 formalized this through the Recovery-Stress Questionnaire framework, which identifies when cumulative stress load exceeds recovery capacity. Halson, 2014 validated these principles in high-performance sport monitoring, and the conclusions apply directly to general population training management. More recently, Starting Strongman reinforced the connection: sleep, stress, and mental health are inseparable variables in long-term strength development.
Phase-specific implications for your clients:
Accumulation phase: Training stress is intentionally high. Life stress must be actively assessed -- a client entering a high-volume accumulation block during a work deadline season is at high risk of stacking physiological stressors. This is the moment to either reduce training volume by 15 to 20 percent or delay the accumulation phase.
Intensification phase: Intensity creates more acute cortisol spikes than volume. A client with elevated chronic stress who is also training at high intensity has a compressed recovery window. HRV monitoring is most diagnostic at this phase.
Deload: The deload is the deliberate stress-reduction event. Its timing should be driven by accumulated fatigue signals, not the calendar -- a client who entered the block with high life stress may need to deload at week four rather than week six.
A recovery-based approach from Frontiers in Physiology, 2026 confirmed through network meta-analysis that managing total stress load -- not just training stress -- is the most significant moderator of post-exercise recovery quality.
Clients reporting persistent sleep disruption, chronic fatigue, or symptoms of clinical stress should be referred to appropriate healthcare providers before recovery programming adjustments are made.
Practical signal: A weekly two-question client check-in -- "Rate your sleep quality, one to ten" and "Rate your life stress level, one to ten" -- provides the allostatic load signal you need to adjust programming in real time.
Need a planning tool to map recovery variables to your client's training phase? The Recovery-Training Integration Template includes the phase-matched sleep, nutrition, and stress load targets for accumulation, intensification, realization, and deload. Download it free below.
Deload Architecture
A deload is a deliberate, structured reduction of training load -- not a "week off" but a programmed phase with specific targets. The distinction matters for client compliance: "rest week" signals optional; "deload block" signals planned and purposeful.
Arnold Schwarzenegger's newsletter -- "Deloading is a Waste of Your Time" (April 7, 2026) -- generated widespread trainer discussion. His cited research argued that muscle protein synthesis peaks post-training and that rest weeks interrupt the adaptation signal. The research is real; the conclusion is partial. The deload debate conflates two different questions: "Should a client take a full rest week?" (contested) and "Should a client reduce volume and intensity by 40 to 60 percent for five to seven days at planned intervals?" (well-supported). The distinction is not trivial. You do not have to choose between training continuity and recovery consolidation. Both belong in the same mesocycle.
The evidence supports structured reduction, not cessation. Research on deloading practices published in Sports Medicine Open, 2024 surveyed 246 competitive athletes and found that all deloaded regularly, with typical deload duration of 6.4 days integrated every 5.6 weeks. Volume was reduced through fewer sets and reps, while training frequency remained unchanged. A complementary study PMC, 2024 confirmed that a one-week deload at the midpoint of a nine-week program produced no negative effect on hypertrophy or endurance outcomes, while allowing systemic fatigue to dissipate. Halson, 2014 documented the same principle in high-performance contexts: structured load reduction maintains adaptation while preventing the accumulation of residual fatigue that degrades performance across blocks.
Phase-specific deload design for your clients:
After accumulation: Full deload -- volume reduced by 50 percent, intensity maintained. This allows recovery from the volume-driven fatigue accumulated over four to six weeks.
After intensification: Partial deload -- volume reduced by 30 percent, intensity reduced by 15 percent. Neural fatigue from high-intensity work requires intensity reduction, not just volume reduction.
During life-stress spikes: Proactive deload triggered by HRV suppression or weekly check-in stress scores, not by calendar.
Recovery periodization directly prevents the six-week hypertrophy plateau -- when sleep, nutrition timing, and stress load are managed alongside volume progression, the adaptation window extends significantly. For more on why programs stall at this inflection point, see Why Most Hypertrophy Programs Fail After 6 Weeks.
Practical signal: Deloads are not earned through exhaustion. They are scheduled through data. A client whose HRV has been suppressed more than 15 percent below baseline for three consecutive days needs a deload now -- not in two weeks when the calendar says so.
The Recovery-Training Integration Model
Understanding the four variables is the prerequisite. Integrating them into a single planning framework that operates alongside the training plan is the skill. Here is the model.
The periodization principles governing training load management apply equally to recovery variable management. The same logic underpinning evidence-based program design -- that training variables must be adjusted by mesocycle phase -- holds for recovery variables. The difference is that most programs only plan one side. Recovery for personal training clients becomes measurably more effective when both sides of the adaptation equation are periodized together.
Matching Recovery to Mesocycle Phase
The table below maps the four recovery variables to each mesocycle phase. This is the post's core practitioner deliverable -- no current training resource publishes a phase-matched recovery variable framework for personal trainers working with general population clients.
What does it look like when all four variables are planned alongside the training block?

The Recovery-Training Integration Framework
Mesocycle Phase | Training Demand | Sleep Target | Nutrition Focus | Stress Tolerance | Deload Trigger |
|---|---|---|---|---|---|
Accumulation (Wks 1-4) | High volume, moderate intensity | 7.5-9 hrs; onset before midnight; protect early NREM | High caloric support; pre-workout carbs; 4+ protein meals/day | LOW -- stacked with high training stress; proactively reduce life obligations | Week 4-5 or when HRV drops >15% from baseline for 3+ consecutive days |
Intensification (Wks 5-8) | Moderate volume, high intensity | 7-8 hrs; pre-sleep cortisol management critical | Shift toward faster-digesting protein post-workout; maintain carbohydrate for session quality | MEDIUM -- intensity generates acute cortisol spikes; monitor cumulative load | Week 7-8 or when session quality (bar speed, rep quality) degrades across 2 consecutive sessions |
Realization (Wks 9-10) | Low volume, peak intensity | 7-8 hrs; sleep schedule consistency (plus or minus 30 min wake time) | Optimize peri-workout nutrition; slightly elevated carbohydrate for peak output | HIGH -- deloaded training stress creates headroom for life stress | Not typically; realization is short (7-10 days) |
Deload | 40-60% volume reduction; intensity maintained | 8-9 hrs target; this phase is the primary recovery consolidation window | Return to baseline fueling; no caloric restriction during deload | RESTORE -- use this phase to actively address accumulated life stress | N/A -- this phase IS the recovery event |
The recovery plan does not replace the training plan -- it overlays it. Your mesocycle structure stays intact; the recovery variable targets change by phase. The client who was training under an accumulation block with high caloric support and 8-plus hours of sleep transitions to an intensification block where sleep architecture quality and cortisol management take priority over raw sleep duration.
The "stress tolerance" column is the least intuitive. During accumulation, training stress is already high, so life stress has the greatest negative impact on adaptation -- there is less headroom in the adaptation budget. During realization, training stress is low (tapered volume), so life stress has the most headroom. This means the same life stressor -- a work deadline, a family obligation -- has a different impact on adaptation depending on the mesocycle phase. Programming must account for that.
The deload trigger column moves the deload from a calendar event to a data-driven event. A calendar deload at week six may be too late for a client whose HRV data showed cumulative suppression starting at week four. It may also be unnecessary for a client whose recovery variables have been well managed throughout the block. The triggers above give you the decision criteria rather than a fixed schedule.
Using HRV as a Programming Input
The table provides phase-level targets. HRV provides the within-phase signal -- the real-time indicator of whether the client's recovery capacity is adequate for the planned training session.
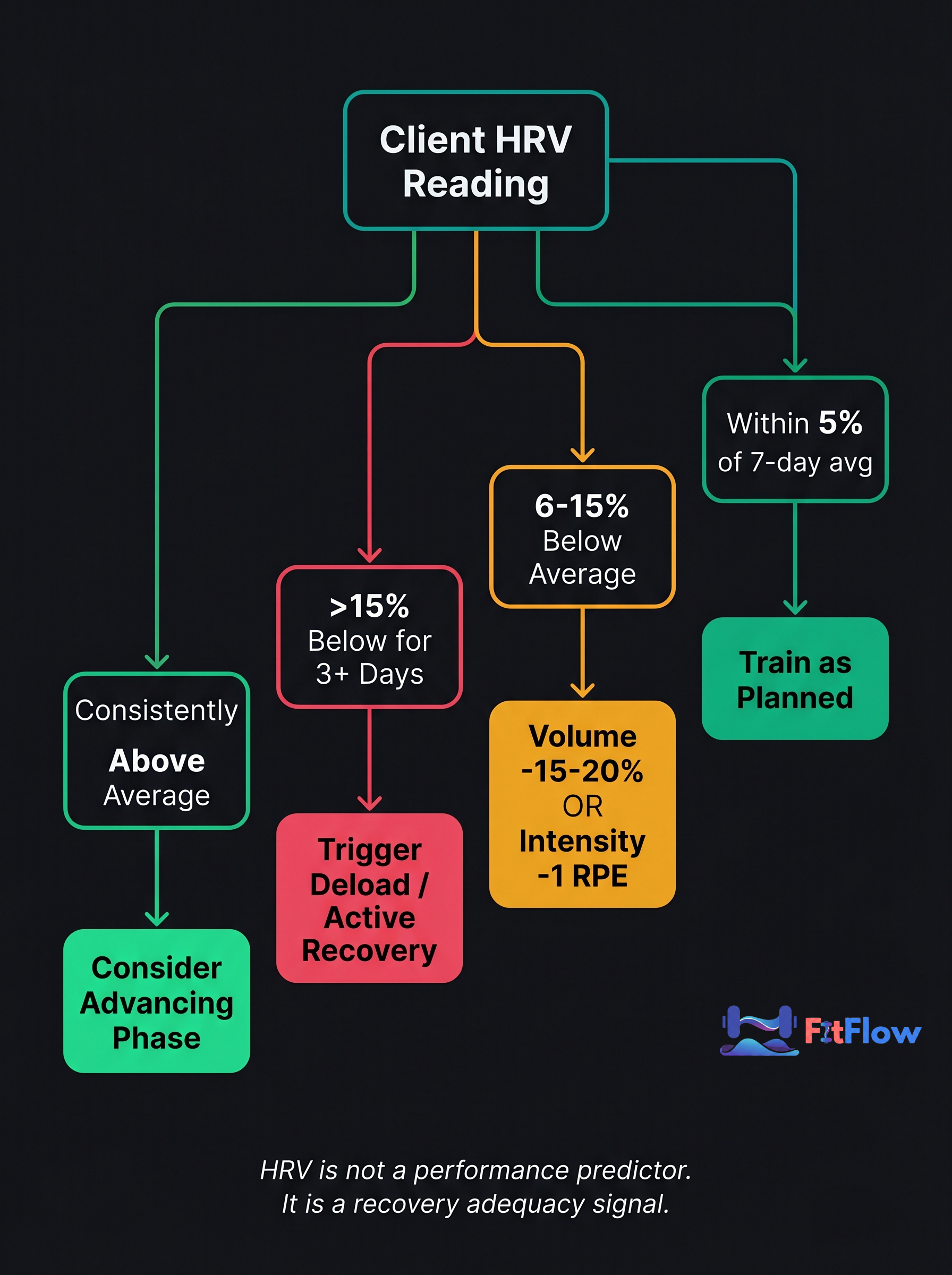
HRV is the variation in time interval between heartbeats, reflecting autonomic nervous system balance between sympathetic (stress-response) and parasympathetic (rest-recovery) activity. Higher HRV indicates stronger parasympathetic dominance and greater adaptation capacity. Lower HRV indicates sympathetic dominance -- the body is still processing prior stress. For trainers, HRV is not a performance predictor. It is a recovery adequacy signal. The question it answers is not "will my client perform well today?" but "is my client's adaptation capacity sufficient to absorb today's planned load?"
The practitioner decision framework:
HRV within 5 percent of the 7-day rolling average: Train as planned. Recovery is adequate.
HRV 6-15 percent below the 7-day average: Reduce session volume by 15 to 20 percent or reduce intensity by one RPE point. Do not skip the session -- the training stimulus is still adaptive; reduce the dose.
HRV more than 15 percent below the 7-day average for 3 or more consecutive days: Trigger early deload or active recovery day. The adaptation budget is depleted; adding training load produces diminishing returns or net fatigue.
HRV consistently elevated above 7-day average: Signal to consider volume progression or intensification ahead of schedule.
The evidence supports this framework. A narrative review of HRV applications in strength and conditioning PMC, 2024 concluded: "There is likely utility to HRV-guided programming compared to predefined programming." The ACSM 2026 Trends Report identified wearable technology as enabling real-time physiological adjustments that improve results and reduce injury risk. The WHOOP 2026 Health Report found that 70 percent of wearable users are already applying data to recovery strategies -- the data exists. Zourdos et al., 2016 validated RIR-based effort management (r = 0.88-0.91), which integrates directly with HRV-guided session modifications for managing training load within recovery constraints. The Trainerize 2026 Trends report confirmed that trainers who translate wearable data into programming decisions gain a measurable competitive edge.
Practical signal: If your client owns a WHOOP, Garmin, or Apple Watch with HRV tracking, those four rules above are the complete decision framework. You do not need a more complex algorithm. You need to act on the signal consistently.
The Weekly Recovery Audit
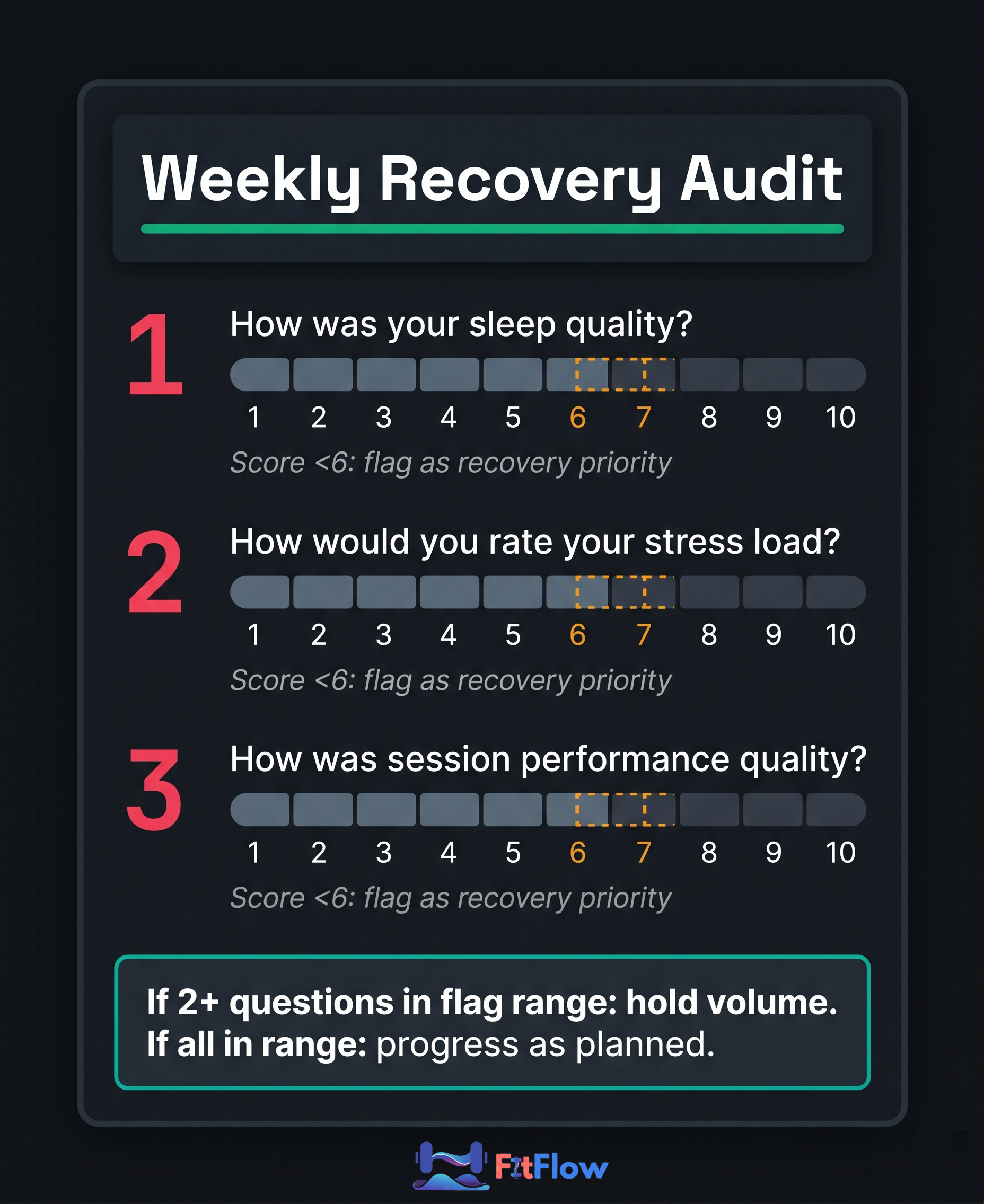
You do not need a wearable data integration dashboard to use this framework. You need five questions answered before each training week begins.
The Weekly Recovery Audit
Sleep quality this week (1-10): If below 6, flag sleep architecture as the recovery priority. Consider reducing accumulation-phase volume by 15 to 20 percent for this week.
Life stress level this week (1-10): If above 7, reduce training stress tolerance accordingly -- shift this week's programming toward technique work, lower RPE targets, shorten sessions.
Training quality last session (1-10): If below 6, do not assume it is a motivation issue. Cross-reference questions one and two. If either is degraded, the performance signal is a recovery signal.
Soreness and fatigue carryover (1-10): If above 7 for two or more consecutive weeks, the training load is exceeding recovery capacity regardless of what the program calls for.
Nutrition compliance this week (1-10): If below 5, the between-session fueling floor has likely been breached. Address substrate availability before adjusting training variables.
Decision rule: If two or more of the five questions score in the flag range, do not add training stimulus this week. Maintain current volume and intensity. If all five are in range, progress as planned.
This is not autoregulation -- it is recovery-informed programming. The training plan stays intact week-to-week; the weekly audit drives minor adjustments within the plan, not to the plan itself.
The WHOOP 2026 Health Report noted that "AI now contextualizes poor sleep based on specific stress loads and recovery patterns." The audit above replicates this logic with a five-question protocol any trainer can implement without wearables. Kellmann et al., 2018 established the Recovery-Stress Questionnaire as the gold standard for monitoring this balance in applied sport settings.
Practical signal: Run the audit at the beginning of each training week. It takes two minutes. It prevents two weeks of wasted programming.
What This Looks Like in Practice
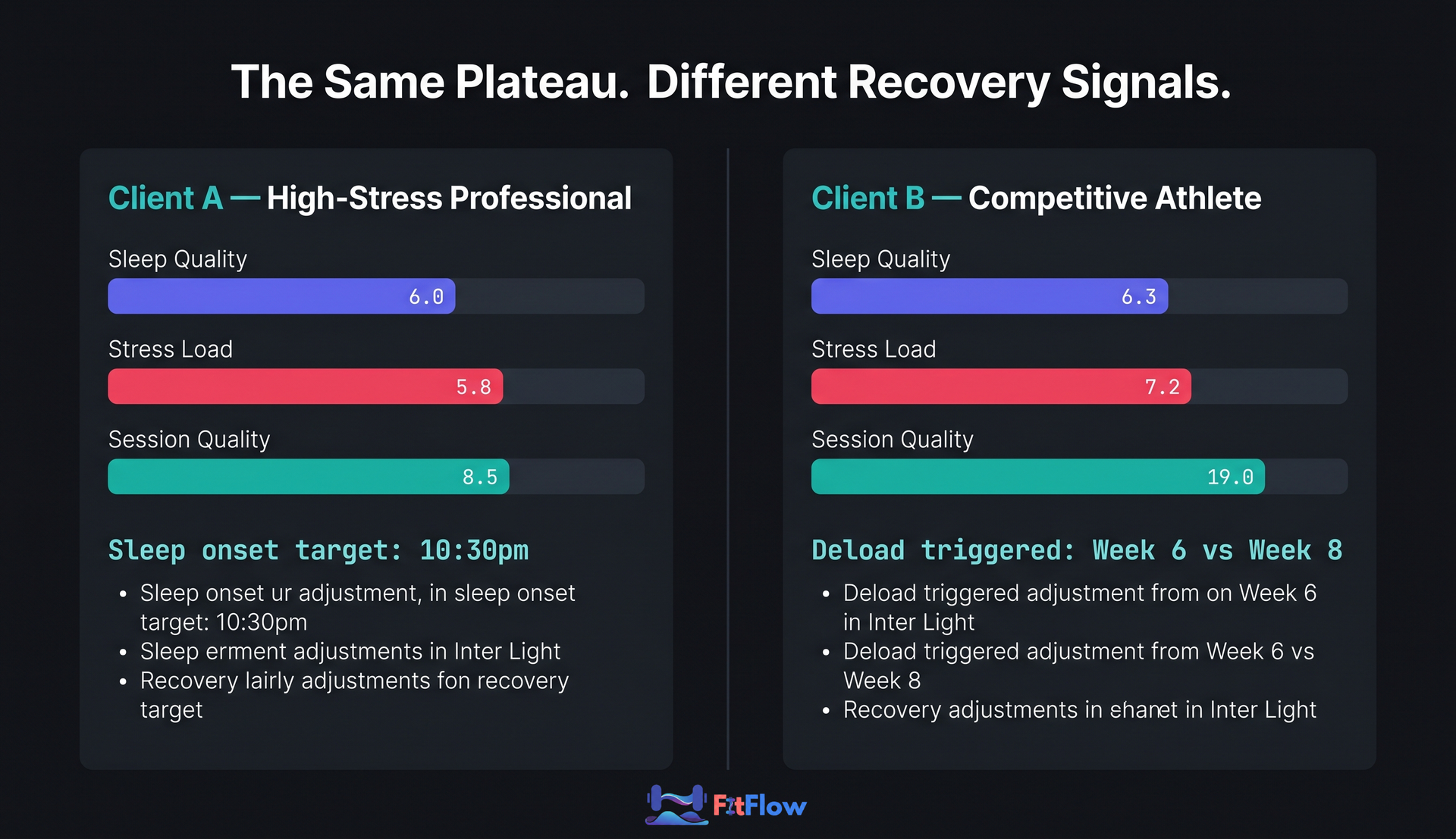
Two client scenarios illustrate how the framework operates under real-world constraints. These are not textbook implementations. They are the kind of situations you encounter on a Tuesday morning when the training log says one thing and the client's physiology says another.
Client A -- High-Stress Professional, 3x/Week
Profile: 38-year-old executive, three training sessions per week, consistently strong motivation. Plateauing on strength gains for eight weeks despite consistent attendance and a well-structured program.
Standard trainer response: Adjust the program -- change exercise selection, add a fourth training day, shift the periodization.
Recovery-periodization response: The weekly audit reveals sleep quality averages 5 out of 10 (wakes at two to three AM most nights) and life stress averages 8 out of 10 (high-demand work season, quarterly board presentations). This client's allostatic budget is nearly fully consumed by non-training stressors. Adding training stress will not produce adaptation; it will compete with recovery for a depleted budget.
Recovery plan adjustments:
Sleep: Establish a pre-sleep protocol targeting early NREM -- lights out by 10:30 PM, no work email after 9 PM, consistent wake time at 6:30 AM daily. The goal is not more sleep hours; it is earlier, more architecture-intact sleep to capture the first NREM GH pulse.
Nutrition: Audit between-session fueling. The pattern in high-stress professionals is predictable: under-eating during the day (busy, meetings, skipping meals), over-eating in the evening. Redistribute protein across four meals. Add a targeted post-workout protein plus carbohydrate meal immediately after each session.
Stress management: Communicate explicitly that this client is not in a phase where adding training volume will help. The current mesocycle must be extended -- not shortened -- until the audit scores normalize. Maintain current intensity and volume; do not progress until sleep quality reaches 7 or above and life stress drops below 6.
The program was not the problem. The recovery substrate was insufficient to convert the training signal into adaptation. Recovery-informed programming, not training-informed programming, resolves the plateau.
Client B -- Competitive Athlete, 5x/Week
Profile: 29-year-old competitive amateur athlete, five training sessions per week, optimizing for performance in a 16-week mesocycle. HRV monitoring via WHOOP. Shows consistent training effort but plateau in intensification-phase performance at weeks six and seven.
Standard trainer response: Assess programming -- re-evaluate volume, intensity distribution, and exercise selection for the intensification block.
Recovery-periodization response: HRV data shows a consistent pattern: HRV is 12 percent below the 7-day rolling average on Wednesdays -- after Monday and Tuesday's sessions. This client is not recovering adequately between sessions two and three of the training week.
Recovery plan adjustments:
Sleep: Session two (Tuesday) produces high neural fatigue from heavy compound lifts. Tuesday evening sleep is the most architecturally critical of the week -- protect it by eliminating Tuesday night social or late work commitments during the intensification phase. Target sleep onset by 10 PM on Tuesdays specifically.
Nutrition: Add a targeted carbohydrate plus protein meal Tuesday post-workout. This client was intermittent fasting post-training. Glycogen resynthesis for Wednesday's session requires immediate post-workout substrate -- the fasting protocol was directly undermining mid-week recovery.
Deload timing: HRV data shows three consecutive Wednesdays with greater than 12 percent suppression. Trigger early deload at week six rather than waiting until the planned week eight. The accumulated fatigue pattern is clear; the calendar is not the appropriate trigger.
This client does not need a different program. The program is appropriate for the mesocycle. The recovery variables were not matched to the training demand of the specific session sequence. Adjusting Tuesday evening recovery and Wednesday pre-session nutrition resolves the mid-week suppression pattern.
Frequently Asked Questions
Comments