Sleep Stacks for Busy Professionals: The 4-Pillar Protocol
Your Executive Client Already Has the Data. They Don't Have a Trainer Who Knows What to Do With It.
The American College of Sports Medicine's 2026 Worldwide Fitness Trends Survey ranked wearable technology #1 for the eighth year running. ACSM's framing: for fitness-interested adults, "the data is already on the wrist." Your high-income executive client walked into their first session with eleven months of Oura sleep stage data, a WHOOP recovery score they check before deciding whether to lift, and an Apple Watch logging HRV every five minutes for two years.
What they don't have is a coach who can convert any of it into a protocol they can execute on a Tuesday with three back-to-back calls and a 7 PM dinner that ends with a wine pairing.
NASM's 2026 Top Fitness Trends Report named this gap directly. Sleep optimization, NASM wrote, has moved "from optional to expected in periodization." The credential bodies have stopped treating sleep as a bonus pillar. In March 2026, ACE published its first full CEU on the subject: Prioritizing Restorative Sleep: The Foundation for Recovery, Resilience and Movement. The permission is official, on letterhead, with CEUs attached.
What remains unbuilt is the delivery system: how a working trainer takes the science, the trends, and the client's wearable data and turns it into a sleep protocol the client will actually run. This article is that delivery system. Four pillars. Twelve depth requirements. Clear scope-of-practice rails. A framework you can hand to your next executive client by Friday.
Why Standard Sleep Advice Fails Busy Professionals
Get the 4-Pillar Sleep Protocol Pack — Free
Most published sleep advice was written for someone with schedule autonomy. Morning walks at 7 AM. Hard 10 PM bedtime. No screens after 8 PM. None of it accounts for the 9 PM board call, the red-eye out of LHR, the founder running on chronically elevated cortisol, or the partner-track lawyer whose Tuesday dinner includes three glasses of Sancerre.
The core insight: for executive clients, sleep optimization is a constraint-management problem, not an education problem. They already know they should sleep more. They have read Walker, watched the Huberman episode, bought the magnesium. The gap is a delivery system that survives contact with their actual calendar.
Huberman gives the DIY stack. ACE gives the permission slip. ISSA gives the business case (a 22% pricing premium for trainers who add recovery specialization, per their 2026 career data). None gives the trainer-delivery framework.
The stakes for the client conversation:
Sleep deprivation reduces muscle protein synthesis by roughly 20-30% in controlled trials — non-trivial for any client paying you to build strength.
Chronically sleep-deprived professionals average 5.5 to 6.5 hours per night.
One night of 4-5 hours of sleep can reduce next-day testosterone in young men by 10-15% (Leproult & Van Cauter, JAMA 2011).
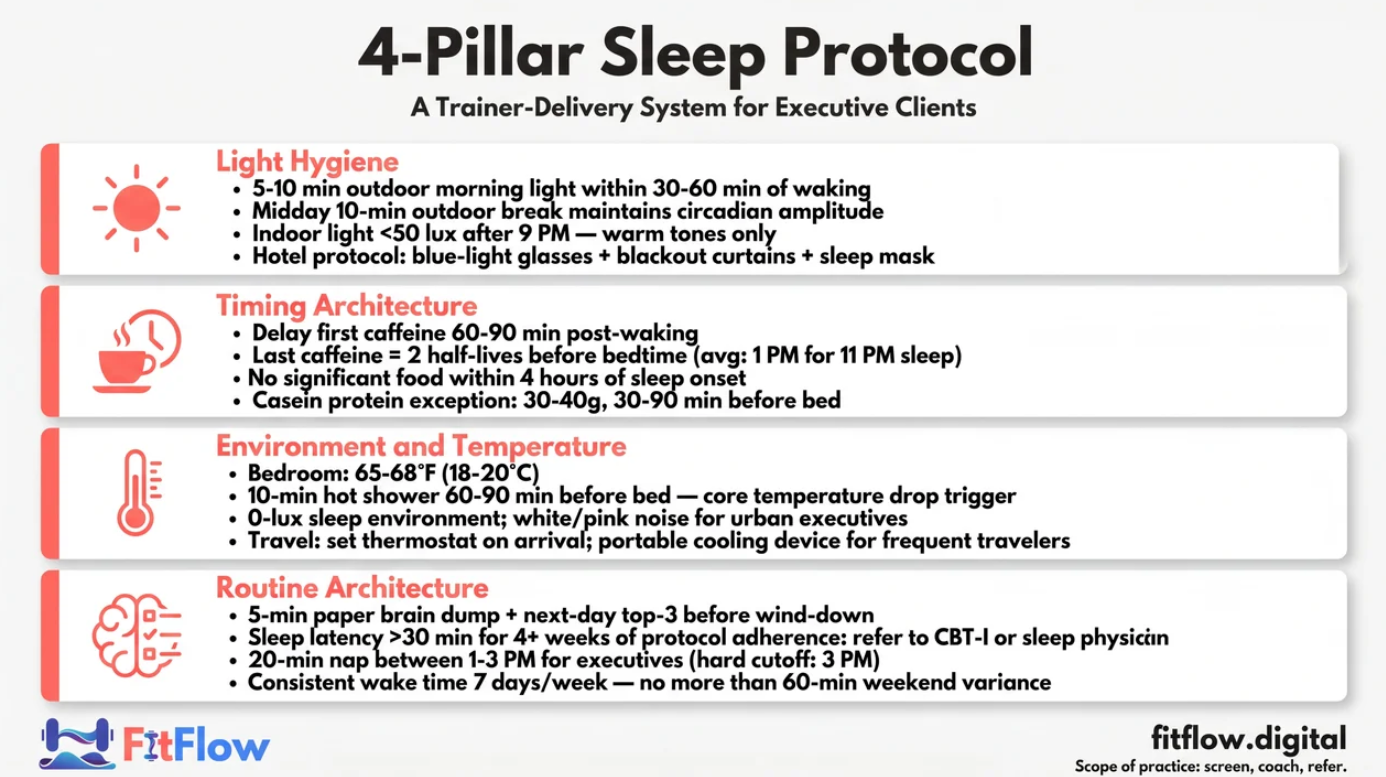
The protocol has four pillars. Each maps to one of two physiological levers. Understand those two levers first.
The Two Levers: Process S + Process C
You don't teach this to your client. You know it so you can frame every intervention.
Process S — Homeostatic Sleep Pressure. Adenosine accumulates across waking hours. The longer awake, the higher the pressure. Caffeine doesn't reduce adenosine — it blocks the receptor, hiding the gauge. When caffeine clears, the pressure hits all at once. That's the "caffeine crash." Every caffeine intervention is a Process S intervention.
Process C — Circadian Process. The internal clock, driven by light and melatonin. Process C controls the 24-hour alerting signal. When Process C alerting drops and Process S pressure is high, the sleep window opens. That overlap is when humans fall asleep efficiently.
Your executive client routinely sabotages both: caffeine stacked until 4 PM (suppresses Process S), overhead office lighting at 8 PM and phone screens at 10:45 PM (delays Process C), and reviewing tomorrow's calendar in bed (activates cortisol). Result: even logging 7 hours, sleep is fragmented, slow-wave low, REM low, and Oura tells them their readiness is 64% for the third morning running.
Two technical numbers:
Adenosine clearance: baseline returns after 7-8 hours of consolidated sleep. Short sleep doesn't fully clear adenosine — which is why sleep debt is real and measurable.
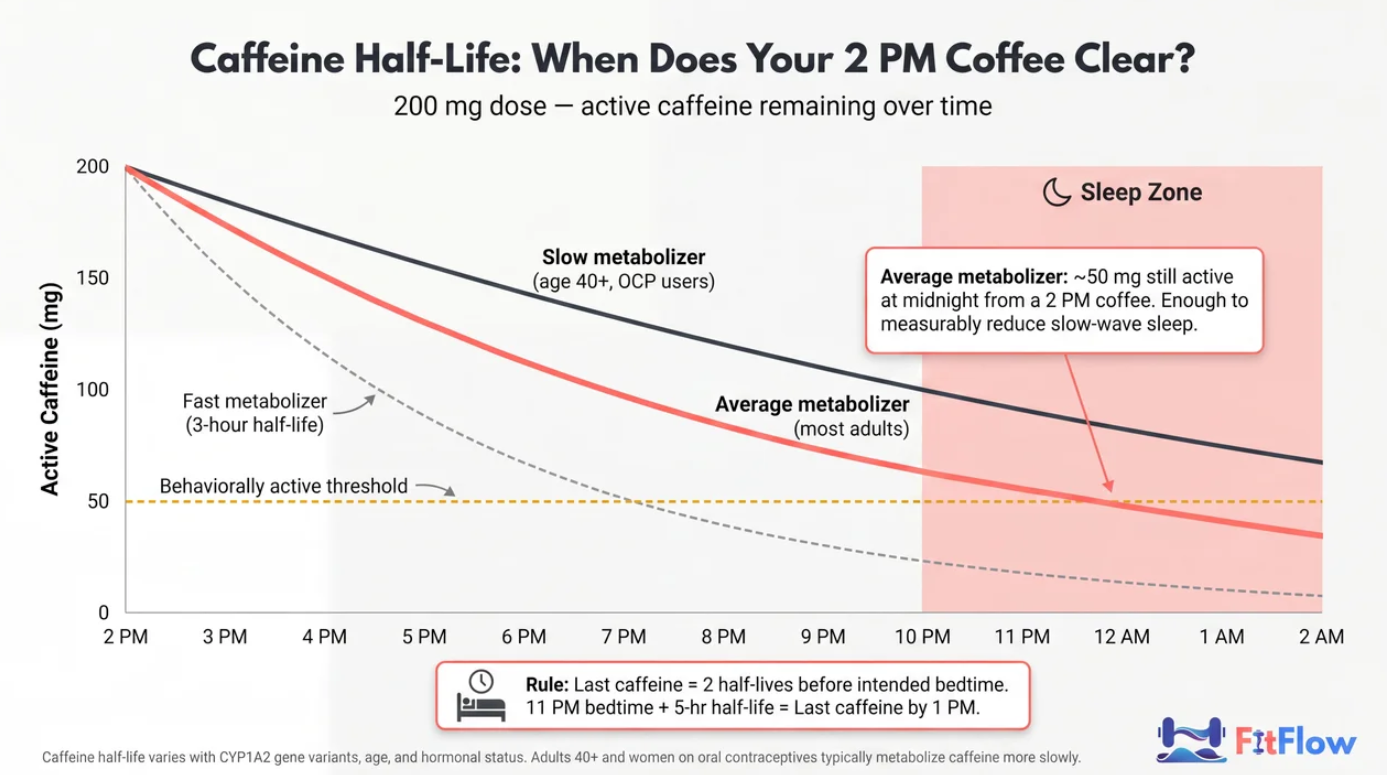
Caffeine half-life: 3-8 hours. Driven by CYP1A2 gene variants, age, and hormonal status. Adults over 40 and women on oral contraceptives metabolize caffeine more slowly. A "2 PM cutoff" rule fails 30-40% of the clients in front of you.
Coach frame: every pillar below is either a Process S management intervention or a Process C entrainment intervention. Label them as such in client communication. The why is what drives adherence.
Pillar 1 — Light Hygiene: The Cheapest Intervention Nobody Does Consistently
Free, zero equipment, highest-leverage circadian intervention. Your client skips it first because it's "too simple."
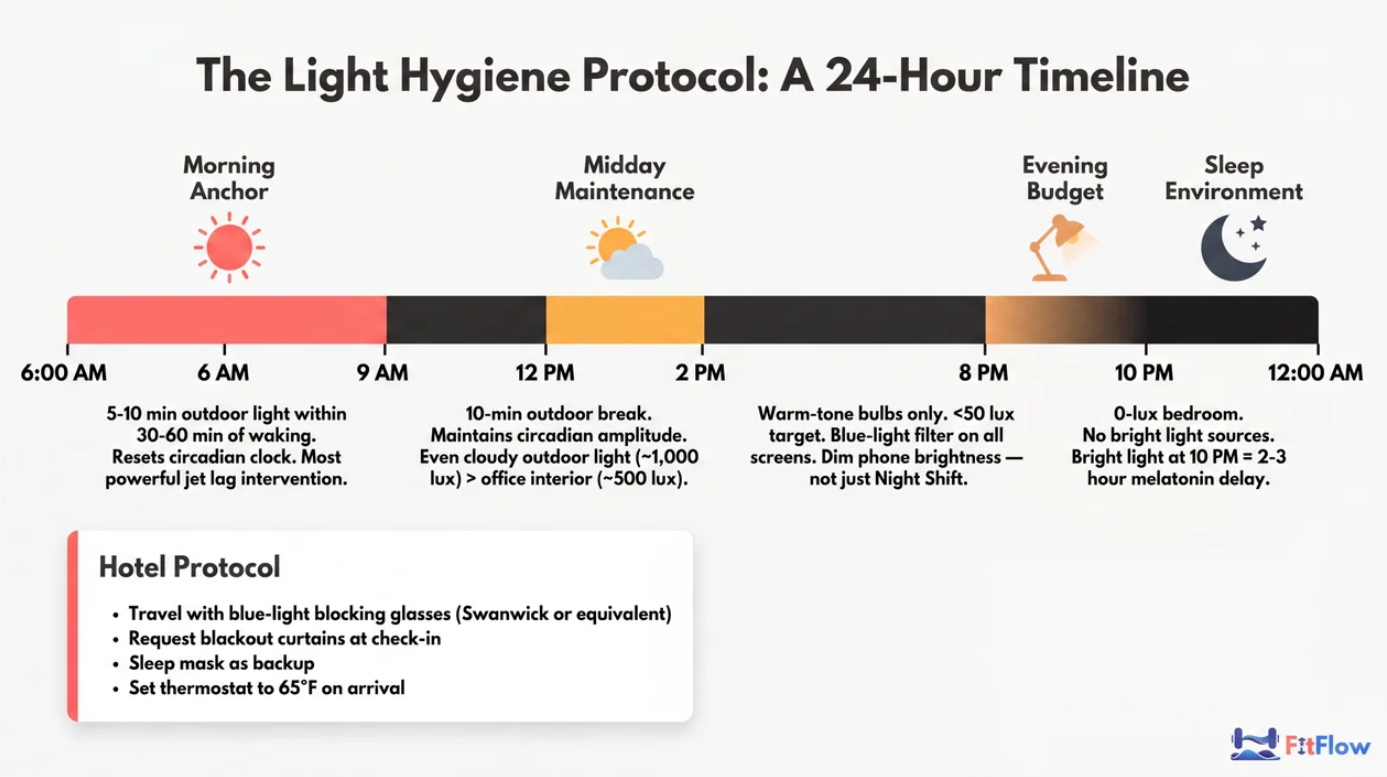
Morning Light Anchor (Process C Entrainment)
Five to ten minutes of direct outdoor light within 30-60 minutes of waking. Not through a window — glass strips most of the relevant short-wavelength spectrum. Outdoor light delivers 1,000-10,000 lux even on overcast days vs. 300-500 lux for indoor office lighting. The order-of-magnitude difference triggers cortisol awakening response and locks circadian phase for the day.
For traveling clients, this is the most powerful jet lag intervention. More reliable than melatonin.
Client script: "Step outside with your first coffee. Five minutes. No sunglasses. If it's still dark at your wake time, use a 10,000 lux light box for fifteen minutes. That's your morning anchor."
Midday Maintenance
Ten-minute outdoor break around noon. It maintains circadian amplitude: the contrast between daytime alerting and nighttime melatonin onset. A flat-amplitude curve produces delayed melatonin onset and longer sleep latency. For windowless-office executives, this is non-negotiable.
Evening Light Budget
After 9 PM, target indoor light below 50 lux. Bright overhead lighting at 10 PM can delay melatonin onset by 2-3 hours. Same magnitude as a moderate caffeine dose.
The practical evening stack:
Warm-tone smart bulbs automated to shift below 2,700K at 9 PM.
Hardware-level screen dimness (not just "Night Shift" color filtering). Pixel brightness drives melanopsin suppression.
For worst offenders, blue-blocking glasses starting at 8 PM.
The Hotel Room Problem
Your client can't control hotel lighting. Build it into the travel protocol: pack a contoured sleep mask and blue-blockers; request blackout curtains at check-in and confirm they fully close; on arrival, immediately set the room to destination-time-zone lighting (lights off and mask on if local bedtime; lights on, curtains open if local daytime). Thirty-second behaviors that produce thirty-minute improvements in sleep onset.
If you're still diagnosing whether sleep is the bottleneck, check the 5 hidden recovery barriers that most trainers miss.
Pillar 2 — Timing Architecture: Caffeine, Eating Windows, and the 4-Hour Rule
This is where executive clients lose 60-90 minutes of sleep latency per week without realizing it.
Caffeine Half-Life Management
At a population-mean 5-hour half-life, a 200 mg coffee at 2 PM leaves 100 mg active at 7 PM and 50 mg at midnight — still enough to measurably reduce slow-wave sleep.
The correct cutoff is two half-lives before intended bedtime. For a client targeting 11 PM lights-out with an average 5-hour half-life, the last dose lands at 1 PM. For a slow metabolizer (over 40, on OCP, known CYP1A2 *2C variant), move the cutoff to noon.
Cortisol-caffeine interaction. Cortisol awakening response peaks 30-60 minutes after waking. Stacking caffeine on the natural peak wastes the adenosine-blocking benefit and amplifies cortisol — a poor trade for an executive already running hot. Better: delay the first coffee 60-90 minutes post-wake, then dose at 10-11 AM and again, if needed, at 1-2 PM as the cortisol curve drops.
The business-meeting workaround. Executives can't decline a 3 PM coffee at a client meeting. Script: "Order a decaf espresso. The ritual is preserved. The caffeine is not."
Pre-Sleep Eating — The 4-Hour Rule
WHOOP published a 2025 analysis in Nature Communications: pre-bed eating within 3 hours of sleep onset degrades HRV and sleep continuity at population scale. The practical rule: no significant caloric intake within 4 hours of intended sleep onset.
Casein protein is the exception. 30-40 g of casein 30-90 minutes pre-sleep supports overnight muscle protein synthesis with negligible HRV penalty in trained individuals.
For executives who entertain late, the workaround isn't abstinence. It's meal composition. High-fat, high-sugar meals within 3 hours of sleep suppress HRV most in the WHOOP dataset. A lighter, protein-forward dinner before 7 PM works better.
Alcohol: The Data
Alcohol is the most misunderstood "sleep aid" in the executive population. It accelerates sleep onset (which clients experience as helpful), then suppresses REM, fragments the second half of the night, and elevates resting heart rate.
WHOOP dose-response data:
Drinks | Sleeping HR | HRV |
|---|---|---|
1 | +1.4% | ~ -8% |
2 | +3.3% | ~ -10% |
3 | +4.3% | ~ -12% |
4 | +6.9% | ~ -15% |
Recovery suppression can persist 4-5 days in collegiate athletes after a single heavy drinking event. Extrapolate conservatively to a 45-year-old founder.
Coaching workaround. Don't frame this as abstinence. Frame it as data literacy. Have the client check their Oura or WHOOP recovery the morning after a drinking night. Twice. After two data points the client makes their own decision. Use the data, not your judgment.
The 4-hour rule applies to alcohol with the same logic. If a client does drink late, a small complex-carb snack may marginally buffer glucose disruption.
Stop Guessing Your Client's Caffeine Cutoff. Get the Timing Card.
Pillar 3 — Environment and Temperature: The Two Dials You Can Control
Bedroom Temperature
Core body temperature must drop 1-3°F from its daytime peak to initiate sleep. An environment too warm inhibits the drop. Target: 65-68°F (18-20°C). Below 60°F triggers shivering arousal; above 70°F delays onset and increases wake-after-sleep-onset events.
For frequent travelers, set hotel thermostat to 65°F on arrival; request extra blankets rather than running warm. For 50+ travel nights per year, a portable cooling device (ChiliPad, Eight Sleep) may help. Some clients report 5-7 point Oura readiness improvement on travel nights.
Pre-Sleep Hot Shower (Paradoxical Core Cooling)
A 10-minute hot shower 60-90 minutes before bed produces peripheral vasodilation. Blood rushes to skin, core temperature drops, and the brain reads the drop as a Process C "begin sleep" signal. Haghayegh et al. meta-analysis: this protocol reduces sleep latency by approximately 10 minutes on average and improves subjective sleep quality.
Client script: "A 10-minute hot shower at 9:30 PM if you want to be asleep by 11. It's a temperature intervention that advances your sleep phase."
The shower marks the start of wind-down and removes the decision of "when do I start getting ready for bed?" Decision fatigue kills executive sleep protocols.
Sound and Darkness
Target 0 lux in the sleep environment; travel mask as default for hotel nights. For urban executives or hotel sleepers, consistent white or pink noise outperforms silence. Pick one app or device and use it nightly.
Pillar 4 — Routine Architecture: Cognitive Offload, Tracking, and the Wind-Down
This pillar covers the final 90 minutes, wearable data interpretation, when napping helps, and how to fix sleep latency vs. total sleep time.
Pre-Sleep Cognitive Offload
The enemy is the default mode network (DMN). Uncompleted tasks dominate working memory and keep the DMN activated. This is why "I'm exhausted but my brain won't shut off."
Baylor University (Scullin et al., 2018): subjects writing a 5-minute "to-do for tomorrow" list before bed fell asleep in an average of 16 minutes vs. 25 minutes for the "completed today" group. The more specific the to-do list, the faster the onset. Cognitive offloading externalizes the open loops and releases the DMN.
Protocol: 5 minutes, pen on paper (not digital — the device pulls them back into work). Brain dump everything still open. Identify tomorrow's top 3 priorities. Close the notebook. This is the final task of the work day, not a bedtime ritual. It runs before the shower.
Don't call this "journaling" to a type-A executive. Call it "closing the browser tabs in your head." Adoption goes from 30% to 80% on the language change alone.
Sleep Latency vs. Total Sleep Time — What to Fix First
Most trainers try to add time in bed first. Backwards. Sleep efficiency (percentage of time in bed actually sleeping) is the primary clinical metric. Fix efficiency before extending time in bed.
Triage:
"I lie awake for 45 minutes before falling asleep." Sleep latency problem. Interventions: consistent bed/wake times, evening light cutoff, hot shower, cognitive offload, address late caffeine.
"I fall asleep fine but I'm still tired." Sleep quality problem (fragmented architecture, low slow-wave, low REM). Interventions: reduce alcohol, manage pre-sleep eating, optimize temperature, screen for OSA.
Sleep latency target: under 20 minutes consistently. If latency exceeds 30 minutes for more than 4 weeks of protocol adherence, refer to CBT-I or a sleep physician.
Sleep Tracker Selection — The Trainer's Decision Guide
Your client is wearing a device. The question is whether you can read the data well enough to use it.
Device | Strength | Limitation | Best For |
|---|---|---|---|
Oura Ring 4 | Near-ECG-grade HR; highest validated accuracy for sleep stages among consumer rings (2025-2026 validation studies); excellent HRV trending; passive form factor | No real-time display; subscription cost | Executive clients wanting professional-grade data without a visible device in meetings |
WHOOP 5.0 | Best-in-class recovery scoring; daily strain/recovery loop built for coaching conversation; strong journaling | Less accurate for sleep staging than Oura in head-to-head testing; subscription-only | Clients in structured training; coaches referencing a daily recovery score in programming |
Apple Watch Series 10+ | Best at wake-time detection; deep iPhone health-data integration; FDA-cleared ECG | Less accurate for deep-sleep staging; battery life can break the overnight loop | Clients already in the Apple ecosystem who won't wear a separate device |
The single most important coaching point on wearables: consumer devices are not polysomnogram-accurate at the sleep-stage level. Recent independent validation shows deep-sleep estimation across all three can be off by 30-50% on any given night. Track trends, not single nights.
HRV trending up or down over a 14-day rolling window?
Recovery score improving as adherence improves?
Sleep onset time stabilizing on consistent wake times?
Single-night data is noise. Two-week trends are signal. This is the most useful framing you can give your client about their own data — and it's the headline of the wearable-interpretation cheat sheet in the Protocol Pack.
Default conversation: "If you already wear a WHOOP or Oura, let's use that data to guide protocol adjustments." Do not mandate device purchase. Use what's there.
Strategic Napping for Executives
Napping is not a crutch. When overnight sleep is constrained by travel or schedule, it's a legitimate cognitive-performance intervention.
Protocol: 20 minutes maximum, set an alarm; between 1:00 and 3:00 PM (the circadian dip window); hard cutoff at 3 PM (later napping reduces homeostatic pressure for the evening sleep window).
A NASA pilot-fatigue study famously found a 26-minute nap improved reaction-time measures by 34%. For executives flying transcon and presenting to a board the same evening, this is performance preservation, not luxury.
The "coffee nap." 200 mg caffeine immediately before the 20-minute nap. Caffeine takes 20-30 minutes to cross the blood-brain barrier; adenosine is partially cleared by the nap; the caffeine then hits a cleared receptor field on waking. Combined effect is meaningfully greater than either alone.
The Wind-Down Stack — The Last 60 Minutes
Hand your client a sequenced timeline. Sequence reduces decision fatigue and runs as a default:
T-90 min: Light dimming begins. No bright overhead light.
T-60 min: Work ends. Cognitive offload (paper brain dump + tomorrow's top 3).
T-45 min: 10-minute hot shower.
T-30 min: Supplements if using (Protocol Pack stack guide: magnesium threonate or bisglycinate 200-400 mg, L-theanine 100-200 mg, glycine 2-3 g — notably no high-dose melatonin for non-jet-lag use). Always consult a physician before starting any supplement regimen.
T-15 min: Reading (physical book or e-ink), light stretching, or breathing (box or 4-7-8).
T-0: Lights out. Consistent wake-time alarm set.
One more rule: do not let the client sleep in more than 60 minutes on weekends. Social jet lag (the gap between weekday and weekend sleep timing) suppresses HRV.
Travel, Jet Lag, and the Road Warrior Protocol
Travel is the most common breakdown point for executive sleep protocols. Build a "travel mode": a subset of the full stack that requires zero equipment.
Direction-specific light: eastward (advancing clock): seek morning light at destination, avoid evening light. Westward (delaying clock): seek evening light, avoid early morning light.
Pre-travel phase shift: for trips crossing more than 3 time zones, shift bedtime by 30 minutes per day, in the direction of travel, for 3 days before departure.
In-flight: hydrate aggressively, no alcohol, no caffeine within 6 hours of destination bedtime. Set watch to destination time zone on boarding. Sleep if it's nighttime at destination, stay awake if it's daytime.
Melatonin as a circadian signal, not a sedative. Executive clients misuse this more than any other supplement.
0.3 to 0.5 mg at destination bedtime resets the circadian clock faster than high doses.
5 mg or higher functions as a sedative, oversaturates receptors, and down-regulates endogenous melatonin production over time.
The 10 mg melatonin gummies from Costco are doing the opposite of what your client thinks. Recommend micro-dose preparations (Pure Encapsulations, Thorne, Momentous all stock 0.3-0.5 mg options). Clients should consult a physician before any new supplement, particularly if on prescription medications.
Recovery timeline: roughly 1 day per time zone for full circadian reset. For a 5-time-zone trip, communicate the 5-day timeline up front. Reduce training load: volume down 30%, intensity down a tier, prioritize sleep over PR attempts during the recovery window.
Sleep Apnea Screening: Essential for Heavy Lifters
The most under-addressed safety topic in trainer-facing sleep content. A competent trainer screening properly can change a client's life.
Why This Matters
Undiagnosed obstructive sleep apnea (OSA) is why some clients "can't sleep well no matter what they do." It's disproportionately common in high-BMI, high-neck-circumference, male, snoring lifters. A trainer who screens and refers appropriately retains the client and may save their life. Untreated OSA links to hypertension, atrial fibrillation, stroke, and increased all-cause mortality.
Scope of Practice
You don't diagnose OSA. You use a validated screening tool to identify risk and refer to the client's physician. NASM explicitly frames the CPT role as part of a "circle of care" — validated screening questionnaires are in scope; diagnosis is not.
STOP-BANG Questionnaire
Two minutes, 8 yes/no questions. STOP-BANG has approximately 93% sensitivity for moderate-to-severe OSA in meta-analytic data (JAMA Network Open):
S — Do you Snore loudly?
T — Often feel Tired, fatigued, or sleepy during the day?
O — Has anyone Observed you stop breathing while you sleep?
P — Do you have or are you treated for high blood Pressure?
B — BMI > 35?
A — Age > 50?
N — Neck circumference > 40 cm (15.7 inches)?
G — Gender = Male?
Score 0-2: low risk. 3-4: intermediate. 5-8: high.
Protocol
Build STOP-BANG into client onboarding intake. For any client scoring 3+ who reports persistently poor sleep quality despite 4+ weeks of adherence, make a direct referral:
"I'd like you to mention your sleep quality to your doctor. There are a couple of specific questions I'd want them to consider — let me send them over."
That language is the language. No diagnosis, no condition named, no fear created.
Why Heavy Lifters Specifically
High-volume strength athletes often develop larger neck circumference even at healthy BMI. Snoring reported by a partner is a significant flag. STOP-BANG triggers earlier in lifters than in the general population — which is why this screen belongs in the strength-coaching intake form.
Red-flag cluster: score 3+, partner-reported snoring, daytime fatigue, sleep duration of 7+ hours that is still non-restorative. Refer. Stop trying to optimize lifestyle when a structural airway obstruction may be the bottleneck.
For the recovery-science foundation that covers sleep alongside nutrition and hydration, see the Evidence-Based Nutrition & Recovery Guide.

When to Refer Out — The Scope-of-Practice Checklist
This is the section that protects you legally and clinically. Be direct, non-apologetic, document the referral.
Refer to a sleep physician when:
STOP-BANG 3+ with reported snoring and daytime fatigue.
Client reports 7+ hours of sleep that is consistently non-restorative for more than 4 weeks.
Sleep latency consistently exceeds 30 minutes despite 4+ weeks of protocol adherence.
Unusual sleep behaviors (sleepwalking, dream enactment, periodic limb movements).
Prescription medication with known sleep interactions (certain antidepressants, beta-blockers, stimulants).
Prior diagnosis of insomnia or any sleep disorder.
Refer to a mental health professional when:
Anxiety or rumination is the primary sleep-onset barrier (beyond typical work stress).
Racing thoughts do not resolve with the cognitive offload protocol.
Depression symptoms co-occur with the sleep complaint.
What to say:
"Your sleep data and what you're describing suggest this may go beyond what I can help you optimize with lifestyle changes. I'd like you to have a conversation with your doctor about a sleep study — it's a simple process and it rules out a physiological factor before we keep adjusting the protocol."
What not to say: do not diagnose, do not name conditions, do not recommend pharmaceuticals, do not suggest supplements as substitutes for physician evaluation.
Documentation: log the referral recommendation in your client file. One line, dated. Your professional record and legal protection.
Bedtime Stacking: The 15-Minute Executive Version
A 2025-2026 TikTok trend called "bedtime stacking" (60-90 minute wind-down rituals filmed for content) has drawn warnings from the American Academy of Sleep Medicine. The criticism: ritualization itself can produce performance anxiety around sleep.
There's truth in bedtime stacking. A pre-sleep sequence reduces decision fatigue and anchors circadian timing. The executive version is 15 minutes:
T-15: Cognitive offload (3 minutes).
T-12: Hot shower (10 minutes).
T-2: Lights out, mask on, room at 65°F.
That's it. No essential oils, no 27-step routine, no camera. Shorter stack = higher adherence = better outcomes.
The Sleep Apnea Screen Most Trainers Don't Know They Can Run. Show Me the Pack.
Key Takeaways
Executive sleep coaching is a constraint-management problem, not education.
Every intervention targets Process S (sleep pressure) or Process C (circadian timing).
Four pillars: Light Hygiene, Timing Architecture, Environment/Temperature, Routine Architecture.
Non-negotiables: morning outdoor light, caffeine cutoff at 2 half-lives before bed, no food within 4 hours of sleep, bedroom at 65-68°F, pre-sleep cognitive offload.
Wearable data: track trends, not single nights. Oura: most accurate sleep stages. WHOOP: best recovery conversation. Apple Watch: best for existing Apple users.
Fix sleep latency before total sleep time.
STOP-BANG screening belongs in every strength-coaching intake. Score 3+ with symptoms = referral.
Travel: 1 day per time zone recovery, direction-specific light, 0.3-0.5 mg melatonin, pre-shift bedtime 3 days out.
Scope of practice matters. Refer out promptly. Document.
Frequently Asked Questions
Comments