Improve Results Without Changing Training. Run This Audit Instead.
Your client has trained four times a week for six months. The program is solid: progressive overload, a sensible split, evidence-based exercise selection. Adherence is 85%. The first 12 weeks produced visible gains. Then results stalled. You know the trainer instinct that fires next — change the program. New split. New exercises. New rep ranges. Maybe a new periodization model. You spend three hours rewriting. Six weeks later, the client is still stalled. You can improve results without changing training, but only if you find the real bottleneck first.
The program is not the bottleneck. The lifestyle around the program is. The 2026 evidence is unambiguous. The American College of Sports Medicine published its first major resistance-training Position Stand in 17 years in March 2026 — a synthesis of 137 systematic reviews and more than 30,000 participants — and explicitly named recovery factors as rate-limiters that can prevent any program from working, no matter how well designed [ACSM 2026 — PMID 41843416]. A February 2026 Sports Medicine dose-response meta-regression (67 studies, 2,058 participants) showed that volume past 12.25 sets per muscle per week adds just 0.24% additional hypertrophy per set [Pelland et al., 2026 — PubMed 41343037]. More program is not the answer.
Two more 2026 signals close the loop. The January 2026 federal dietary guidelines made 1.6 g/kg the official daily protein floor, and most clients are below it four to five days a week. The 2025 REDS-S consensus update extended energy-availability screening from elite athletes to recreational lifters: below 30 kcal per kg of fat-free mass per day, results break regardless of program quality. Sleep, energy, protein — not periodization, not exercise rotation, not split selection — are the variables now rate-limiting your stalled clients.
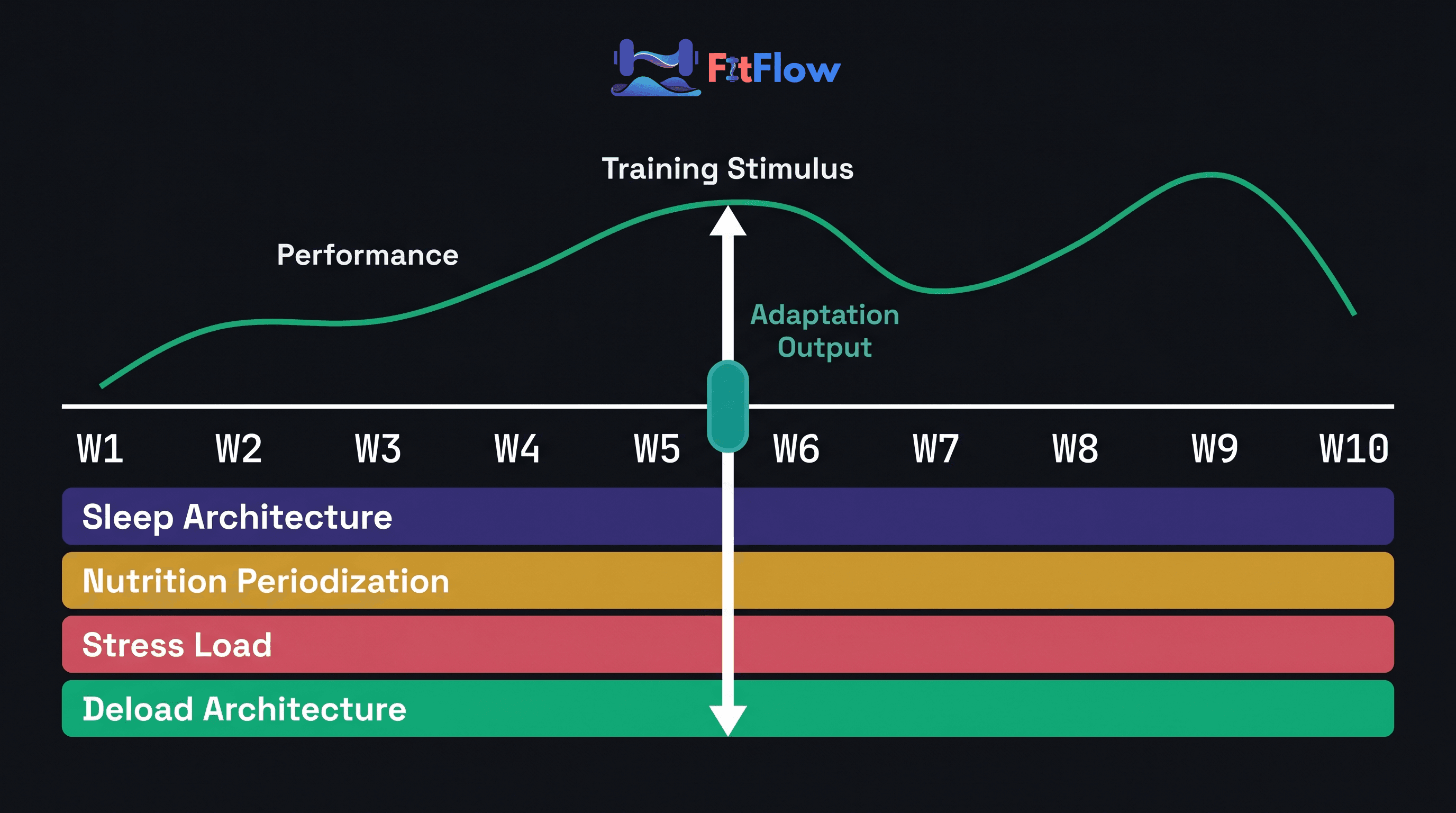
Seven non-training variables drive most off-program stalls. They are ranked below by evidence-weighted impact, anchored to the 2026 thresholds, and assembled into a 6-step audit you can run with any client in 20 minutes. We previously ranked the variables INSIDE the program in The 80/20 of Training Results. This post ranks the variables OUTSIDE it. Together they form a before-you-change-the-program / after-the-program-is-dialed-in diagnostic loop. This post is the audit complement to Recovery as a Growth Lever — ranked, threshold-anchored, and operational, not framing-level.
We built the Off-Program Audit: 20 questions across the 7 lifestyle domains that reveal which variable is capping each client's results. Download it free at the bottom of this article.
Why Most Plateaus Aren't Programming Plateaus
The Evidence Says the Program Isn't the Bottleneck
The ACSM 2026 Position Stand named recovery factors — sleep, nutrition adequacy, between-session rest — as rate-limiters that can prevent any program from working, no matter how well designed [ACSM 2026 — PMID 41843416]. The institution that writes the official guidelines now says the inside-the-program optimization gain is small; recovery substrate is what determines whether any of it converts into adaptation. The same Position Stand declared that consistency beats complexity, training to failure is not required for strength or hypertrophy gains, and periodization models do not consistently outperform one another for the average adult.
Pelland et al. 2026 Sports Medicine dose-response meta-regression (67 studies, 2,058 participants) put a number on the diminishing-returns curve: hypertrophy plateaus at approximately 12.25 sets per muscle per week, after which each additional set adds 0.24% growth — a tight regression coefficient, not a generalization [Pelland et al., 2026 — PubMed 41343037]. The curve was first mapped earlier [Schoenfeld et al., 2017 — PubMed 28498672]; the 2026 update made it precise. Past 12 sets, the inside-the-program lever is mathematically near-zero.
Field-scale data tightens the conclusion. James Steele's 15,000-participant, 7-year cohort produced 30-50% strength gains on roughly 20 minutes per week of consistent training, as reported in NPR's January 2026 minimum-dose series drawing on Steele et al. [Steele et al. — cohort summary]. Minimum-dose programs work because adherence multiplied by an intact lifestyle substrate produces most of the available adaptation. Pak & Schoenfeld 2025 (Train Smarter, Not Longer; ISBN 1718239297) makes the same case at book length.
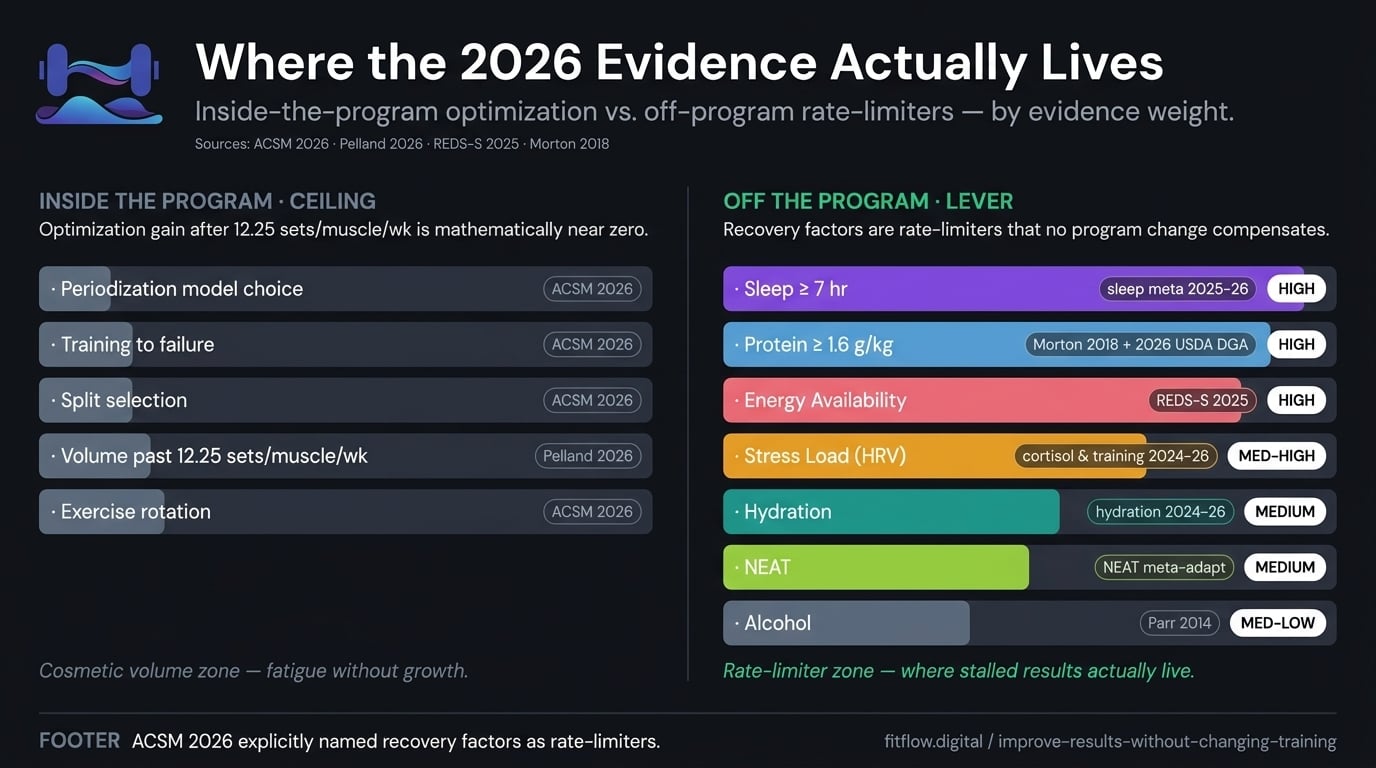
The 2026 evidence converges: when the program is consistent and progressive, the bottleneck is rarely the program. The ACSM 2026 Position Stand names recovery factors as rate-limiters; the 2026 Sports Medicine meta-regression shows volume past 12.25 sets per muscle per week adds 0.24% per set. The OUTSIDE-the-program 20% — sleep, protein, energy availability, stress — is where stalled results actually live.
If volume above 12 sets a week barely moves the needle and failure is not required, a better program is not the missing variable. The missing variable lives in the 23 hours per day the client is not training.
The 70/30 Rule, Operationalized
Trainers in 2026 say nutrition and lifestyle drive 70 percent of results, training drives 30. The Trainerize 2026 State of the Industry report named habit-and-behavior coaching a top trend of the year. The 70/30 rule has hardened into the dominant frame in the trainer feed. Almost no one has converted the talking point into a tool.
This post operationalizes the rule. We rank the seven variables that make up the 70 percent, anchor each to a 2026 quantitative threshold, and assemble them into a 20-question diagnostic that runs in 20-30 minutes per client. The talking point becomes a procedure.
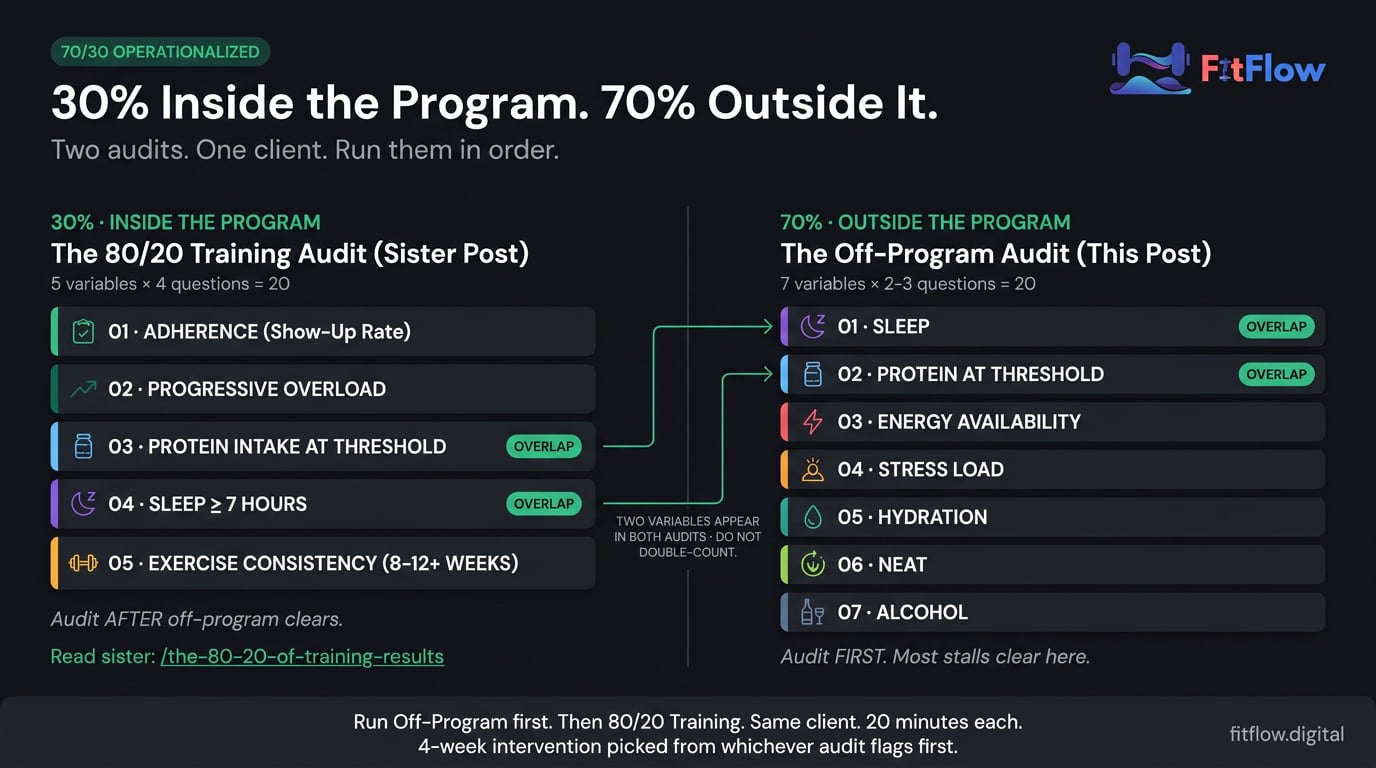
We did the same thing for the 30 percent in The 80/20 of Training Results. The two posts are an explicit sister-pair: before you change the program, run THIS audit; after the program is dialed in, the 80/20 is the maintenance check. For Sam, this is the conversation that protects margin — 20 minutes to run the audit, then a 4-week intervention on the highest-ranked flagged variable. For Eric, this is the answer to "should I buy a new program?" — almost always, no.
The Off-Program Leverage Hierarchy: 7 Variables That Drive Stalled Results

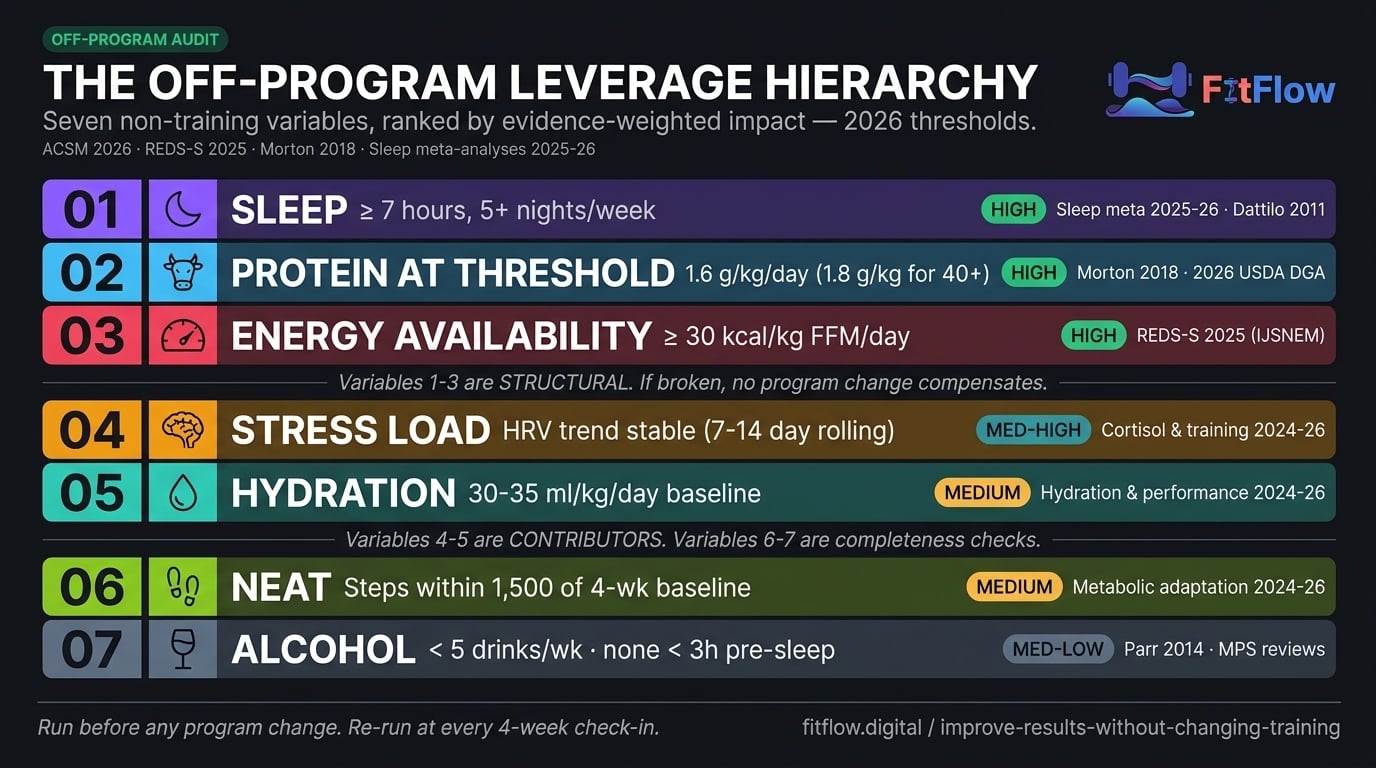
Seven non-training variables carry the overwhelming majority of off-program stalls. They are ranked below by evidence-weighted impact, anchored to 2026 thresholds where consensus exists. Variables 1-3 are the structural floor: if any is broken, no program change will fix what it is capping. Variables 4-5 are common contributors. Variables 6-7 are smaller levers, useful for completeness.
Rank | Variable | Evidence Weight | 2026 Threshold | When It Is the Lever |
|---|---|---|---|---|
1 | Sleep | HIGH | 7-hour floor, 5+ nights/week | Always check first. 3+ nights below 7 hours triggers the lever. |
2 | Protein at Threshold | HIGH | 1.6 g/kg/day (1.8 for clients 40+) | Sleep clears but adaptation lags. Average <1.4 g/kg flags it. |
3 | Energy Availability | HIGH | <30 kcal/kg FFM/day = high risk | Sleep + protein clear but client reports fatigue, mood, cycle changes. |
4 | Stress Load | MEDIUM-HIGH | HRV trend declining 3+ weeks | Ranks 1-3 clear but performance/RPE declines. |
5 | Hydration | MEDIUM | 30-35 ml/kg/day baseline | Lethargy, low intake (<25 ml/kg), hot/humid environments. |
6 | NEAT | MEDIUM | Steps within 1,500 of 4-week-prior baseline | Body-composition phase + sustained deficit + step count fallen. |
7 | Alcohol | MEDIUM-LOW | Behavior: <5 drinks/week, none within 3h of bedtime (mechanistic floor: <0.5 g/kg per session) | Weekly intake >5 drinks or pre-sleep alcohol on training days. |
Evidence weights: HIGH = meta-analyses + 2026 guideline / consensus position. MEDIUM-HIGH = strong mechanistic + active 2024-2026 review consensus. MEDIUM = systematic review support with calibration debate. MEDIUM-LOW = solid mechanism, smaller typical effect size.
1. Sleep — Evidence Weight: HIGH (Threshold: 7-Hour Floor, 5+ Nights/Week)
Seven or more hours of sleep per night, sustained on at least five of seven nights, supports the hormonal, neurological, and tissue-repair substrate on which training adapts. Below the 7-hour floor, strength expression, hypertrophy response, and reaction time all degrade measurably. Below 6.5 hours for three or more consecutive nights, adaptation is meaningfully impaired.
The 2025-2026 sleep-and-performance literature has converged on the 7-hour floor (Walsh et al. 2025 in IJSPP; Charest & Grandner 2025; Sports Medicine and Journal of Sleep Research systematic reviews). Foundational citations: Dattilo et al., 2011 — PMID 21550729; Chennaoui et al., 2015 — PMID 25127157. Sleep extension trials (an extra hour vs. baseline) produce 3-9% strength gains in athletes, larger than most program tweaks deliver.
Sleep ranks first because it is the substrate on which every other variable operates. Below 6.5 hours, protein ingestion produces less protein synthesis, energy availability appears worse than it is, stress responses are amplified, and hydration cues are suppressed. Sleep is the rate-limiter that breaks the other rate-limiters.
When it is the lever: always check first. Practical signal: ask for average sleep duration across the past 7 days and how many nights were below 7 hours. Three or more nights below 7 hours and sleep is the bottleneck. Below 6.5 hours sustained, no program or nutrition change will produce progress.
Refer-out guardrail (sleep disorders): If a client reports symptoms consistent with sleep apnea (snoring + daytime fatigue + observed apnea episodes), insomnia of more than three months despite hygiene intervention, or restless legs syndrome, refer to a sleep medicine specialist. Coach hygiene; do not diagnose disorders.
For the recovery-failure pattern as a whole, see the diagnostic deep-dive: Why Your Clients Are Not Recovering. Sleep is also rank 4 in the inside-the-program hierarchy — see the sleep section of The 80/20 of Training Results for how the inside-the-program and outside-the-program perspectives align.
2. Protein at Threshold — Evidence Weight: HIGH (Threshold: 1.6 g/kg/day, 1.8 g/kg for 40+)
The threshold is 1.6 grams of protein per kilogram of body weight per day, distributed across three to five feedings: the dose-response threshold for resistance-training-induced hypertrophy and strength retention. For clients aged 40 and older, the threshold rises to roughly 1.8 g/kg to overcome anabolic resistance.
Morton et al., 2018 — PMID 28698222 is the anchor: a meta-analysis of 49 studies and 1,863 participants that established 1.6 g/kg. Q1 2026 protein meta-regression updates confirm the threshold and refine the 40+ adjustment. The January 2026 federal dietary guidelines codified 1.6 g/kg as the official US recommendation. The fitness industry has been at this number since 2018, but the federal-policy validation is what made it newsworthy.
Protein ranks second because the evidence is rock-solid (stable for eight-plus years), the gap between client behavior and threshold is enormous (most clients hit it 2-3 of 7 days), and closing the gap is operationally cheap (one habit shift — "protein at every meal" — usually solves it).
When it is the lever: sleep clears but adaptation lags. Practical signal: ask for 24-hour protein intake on three recent days. An average below 1.4 g/kg flags protein as the lever. Below 1.2 g/kg, protein is almost certainly the dominant lever for the next four-week block.
Refer-out guardrail (chronic kidney disease): Clients with diagnosed CKD or other renal conditions require individualized protein guidance from a dietitian or nephrologist. The 1.6 g/kg threshold applies to healthy adult clients.
For the practical protein-coaching framework and plate methods, see the deep-dive: Simple Nutrition Frameworks for Training Clients. Protein is rank 3 in the inside-the-program hierarchy — see the protein section of The 80/20 of Training Results.
3. Energy Availability — Evidence Weight: HIGH (Threshold: <30 kcal/kg FFM/day = High Risk)
Energy availability (EA) = (energy intake − exercise energy expenditure) / fat-free mass, in kcal/kg FFM/day. The 2025 REDS-S consensus thresholds: <30 = high risk for adaptation impairment; 30-45 = moderate; >45 = adequate.
The 2025 REDS-S consensus update (IJSNEM) formalized the REDS-Scoring system and, critically, extended the framework from elite athletes to recreational lifters and training clients. The 2018 IOC consensus applied to elite endurance and aesthetic-sport athletes; the 2025 update applies to general fitness populations. Most trainers do not yet know about this extension. For intellectual honesty, the threshold is calibration-debated: Heikura et al., 2021 — PMID 34296227 found <30 kcal/kg FFM may not apply cleanly to non-elite endurance males.
Energy availability ranks third because it is the single most under-audited variable in trainer practice. EA is the likely bottleneck for clients in a body-composition phase, with high training volume relative to caloric intake, female clients with cycle disturbances, or any client reporting fatigue plus adaptation failure despite adequate sleep and protein. Your certification taught you to write programs. Nobody taught you to audit the substrate the program operates on.
When it is the lever: sleep and protein clear but the client reports fatigue, low libido, mood or sleep disturbances, cycle changes, recurrent illness, or stalled body composition. Practical signal: estimate caloric intake (3-day food log) and exercise energy expenditure (session minutes × MET load). Divide net by fat-free mass. Below 30 kcal/kg FFM/day, EA is the lever.
Refer-out guardrail (REDS-S high-risk): If a client screens at <30 kcal/kg FFM/day energy availability, refer to a registered dietitian or sports physician. Trainers should not attempt sustained EA intervention solo. Document the screen, escalate to a credentialed clinician, and resume training programming once a nutrition plan is in place. The REDS-S high-risk window is at the edge of trainer scope of practice.
For the comprehensive nutrition science underpinning energy availability, see the pillar reference: Evidence-Based Nutrition & Recovery Guide.

4. Stress Load — Evidence Weight: MEDIUM-HIGH (Stress-Bucket Model, Not Cortisol Panic)
Total stress load = life stress (work, sleep deprivation, psychosocial) + training stress + recovery deficit. When the bucket overflows, training adaptation degrades regardless of program quality. This is the stress-bucket model, not the cortisol-fearmongering model that dominated 2025-era influencer content.
The 2026 "stop blaming cortisol" backlash is the corrective signal. Acute cortisol elevations during training are normal and adaptive; chronic baseline elevation under sustained life stress is the actual mechanism. Coach the actual stress inputs — sleep, training load, life stress — not the supplement stack.
HRV (heart rate variability) is the most accessible field measure. The trend across 7-14 days carries the signal, not the absolute number. Wearable accuracy is variable: Oura Gen 4 leads 2026 HRV validation while Whoop and Apple Watch lag, though both produce usable trends. Use the trend, not the score. See Wearable Data Problems.
Stress load ranks fourth because it is partially outside the trainer's control and the screening signal is noisy. But it ranks above hydration, NEAT, and alcohol because when it is the bottleneck, no other intervention compensates. When it is the lever: ranks 1-3 clear but the client reports declining performance, elevated RPE at prior loads, mood changes, or sleep disruption. If HRV trend is declining three or more weeks AND perceived stress is high, stress load is the lever.
Refer-out guardrail (mental health): If a client reports persistent low mood, suicidal ideation, anxiety that interferes with daily function, or disordered eating behaviors, refer to a mental health professional. Trainers can support the lifestyle inputs (sleep hygiene, training load adjustment) but should not attempt to substitute for clinical care.
5. Hydration — Evidence Weight: MEDIUM (Threshold: 30-35 ml/kg/day Baseline + Sweat-Loss Adjustment)
The threshold is 30-35 ml of fluid per kg of body weight per day as baseline, with adjustments for sweat loss (typically 500-1,000 ml extra per training hour in moderate climates). Mild dehydration of 1-2% body mass loss consistently degrades strength and aerobic performance in 2024-2026 reviews.
Hydration ranks fifth because it is rarely the SOLE bottleneck. Clients with chronically poor hydration usually also have poor sleep or poor energy availability, and the intervention is operationally simple. It ranks above NEAT and alcohol because it affects strength clients across all body-composition phases.
When it is the lever: client reports lethargy, headache, or constipation; trains in hot or humid environments without a hydration plan; caffeine or alcohol intake is high while water intake is low. Practical signal: 24-hour fluid intake vs. 30-35 ml/kg baseline plus a urine color check. Below 25 ml/kg, hydration is contributing. For the comprehensive hydration framework, see Evidence-Based Nutrition & Recovery Guide.
6. NEAT (Non-Exercise Activity Thermogenesis) — Evidence Weight: MEDIUM (Most Relevant for Body-Composition Clients)
NEAT is all physical activity outside structured exercise: walking, fidgeting, occupational movement, household tasks. NEAT can vary 200-2,000+ kcal/day across individuals (Levine, 2002). NEAT compensates downward by 20-40% during caloric deficits, the metabolic-adaptation mechanism (MacLean et al., 2011). The TikTok 10K-step trend is directionally correct: maintaining baseline NEAT (8-12K steps/day) protects body-composition outcomes during a deficit.
NEAT ranks sixth because it is most relevant for body-composition clients in a deficit, and the intervention is highly individual. When it is the lever: body-composition phase, sustained deficit four or more weeks, stalled fat loss despite adherent calories. Practical signal: 7-day average step count vs. 4-week-prior baseline. Steps fallen 1,500 or more per day = NEAT is contributing.
7. Alcohol — Evidence Weight: MEDIUM-LOW (Behavior Threshold: <5 drinks/week; Mechanistic Floor: <0.5 g/kg per session)
Acute alcohol consumption above 0.5 g/kg body weight (roughly 3 standard drinks for an 80 kg adult) suppresses post-exercise muscle protein synthesis by 24-37% for 24-48 hours. Chronic moderate consumption (5+ drinks/week) measurably reduces strength gains over 12-week cycles. Parr et al., 2014 — PLOS One is the foundational citation. Sleep architecture is also degraded by alcohol consumed within three hours of bedtime, compounding with rank 1.
Alcohol ranks seventh because most clients can self-correct once aware, and for clients drinking under two drinks per week, it is rarely the primary bottleneck. When it is the lever: five or more drinks per week, drinks within three hours of bedtime, or noticed performance changes after social events. Practical signal: 7-day alcohol intake. More than 5 drinks per week, or two-plus drinks within 3h of bedtime on training days, and alcohol is contributing.
Refer-out guardrail (disordered eating, cross-cutting): If audit responses suggest disordered eating patterns (extreme caloric restriction with high training volume, body dysmorphia, compensatory exercise, or compensatory drinking patterns), refer to a clinician with eating disorder expertise. The Off-Program Audit is a coaching tool, not a clinical assessment.
What You Can Safely Deprioritize
If seven variables carry most of the off-program weight, several recovery and lifestyle interventions you may be coaching to clients carry almost none. These are the recovery and supplementation behaviors that feel productive but do not meaningfully change outcomes for the typical client. Let them go.
Cold plunges, ice baths, and contrast therapy as routine recovery. The 2024-2026 reviews show post-training cold immersion BLUNTS hypertrophic and strength adaptation in resistance-trained populations (Fyfe et al. 2019 / 2024 follow-up). For your strength and hypertrophy clients, skip the post-session cold plunge. It feels recovery; it costs adaptation.
Cortisol-management supplements (ashwagandha, rhodiola, adaptogens). Effect sizes in 2024-2026 reviews are small to non-existent at typical doses. Coach the actual stress inputs (sleep, training load, life stress); skip the supplement stack.
Foam rolling for "recovery" beyond the warm-up benefit. Acute mobility benefit, no measurable downstream effect on hypertrophy, strength, or recovery markers (2024 systematic reviews). Use it for warm-up if the client likes it; do not coach it as a recovery intervention.
Tracking HRV daily and reacting to the score. Day-to-day HRV variation is noisy. The TREND across 7-14 days carries the signal; the daily score does not. Stop coaching reactive program changes off a single morning HRV reading. See Wearable Data Problems for the trend-vs-score discipline.
Carb-cycling, IF windows, "metabolic flexibility" protocols, and timing-precision interventions for clients who have not yet hit the protein floor. When the client is below 1.4 g/kg protein four days a week, advanced timing protocols are theater. Hit the floor first. See Why Perfect Diets Fail for the adherence-over-precision frame in nutrition.
None of these are wrong under every circumstance. Under elite-client demands or specific advanced contexts, they may matter at the margin. But for 80%+ of clients on a typical trainer's roster, coaching them BEFORE the seven ranked variables is upstream noise. You can stop coaching this. That is not a concession; it is a reallocation.
Diagnose Which of the 7 Variables Is Capping a Specific Client in 20 Minutes. You just read the seven variables. The Off-Program Audit turns that hierarchy into a 20-question diagnostic you can run at every client check-in — with pass/borderline/fail thresholds tied to peer-reviewed evidence, a rank-ordering worksheet that picks the single highest-priority intervention, an intervention decision tree with 5 refer-out guardrails (REDS-S, mental health, sleep disorders, CKD, eating disorders), and a 4-week intervention template per variable. Download the Free Audit.
How to Run the Off-Program Audit
The Off-Program Audit is a 6-step procedure to diagnose which of the seven lifestyle variables is capping a specific client's results. Run it before any program change, at every 4-week check-in for plateaued clients, and on every new client at intake. The audit takes 20-30 minutes and ends with a ranked intervention plan.
Step 1: Screen sleep. Ask for sleep duration across the past seven nights. Count nights below 7 hours. If three or more, sleep is the lever — stop the audit and run a 4-week sleep-floor intervention before changing anything else. If fewer, continue.
Step 2: Screen protein. Have the client estimate 24-hour protein intake for three recent days. If the average is below 1.4 g/kg/day (1.6 for clients 40+), protein is the lever. Coach the protein floor for four weeks before any program change. If at threshold, continue.
Step 3: Screen energy availability. For body-composition phase, high training volume, female clients with cycle disturbances, or any client reporting fatigue plus low libido plus mood changes: calculate EA = (caloric intake − exercise energy expenditure) / fat-free mass. If <30 kcal/kg FFM/day, refer out to a registered dietitian or sports physician (scope-of-practice boundary). If 30-45, flag as moderate risk. If >45, continue.
Step 4: Screen stress load. Use a 7-14 day HRV trend plus a 7-day perceived-stress self-report. If HRV trend is declining three or more weeks AND perceived stress is high, stress load is the lever. Adjust training volume downward 20% for two weeks, coach sleep and life-stress inputs, re-screen.
Step 5: Screen hydration, NEAT, and alcohol. Hydration: 24-hour fluid intake versus 30-35 ml/kg baseline. NEAT: 7-day step average versus 4-week-prior baseline (body-composition clients in a deficit only). Alcohol: 7-day intake; flag if more than 5 drinks per week or two-plus drinks within 3h of bedtime on training days.
Step 6: Rank-order findings and pick ONE intervention. Work in rank order: sleep first, then protein, then EA (refer-out), then stress, then hydration / NEAT / alcohol. Do NOT change more than one variable at a time, and do NOT change the program in parallel. A 4-week clean intervention on the highest-ranked flagged variable produces the cleanest cause-and-effect signal.
The lead magnet below walks through 20 specific diagnostic questions across these six steps — two to three per variable — printable for in-session use with each client.
Conclusion
When a client stalls and the program is solid, the trainer's instinct is to change the program. The 2026 evidence says the program is not the bottleneck — seven non-training variables are. The ACSM 2026 Position Stand named recovery factors as rate-limiters [ACSM 2026]. The 2026 federal dietary guidelines codified the 1.6 g/kg protein floor. The 2025 REDS-S consensus extended energy-availability screening to recreational lifters. The 2025-2026 sleep literature converged on the 7-hour floor. Sleep, protein, energy availability, stress, hydration, NEAT, alcohol — ranked, threshold-anchored, audit-ready. To improve results without changing training, run the audit before you change the program.
For Scaling Trainer Sam: this quarter, run the Off-Program Audit on every plateaued client BEFORE rewriting their program. Most stalls clear with a single 4-week intervention on a non-training variable, usually sleep or protein. That protects your delivery margin (20 minutes per audit, no programming complexity added) and turns "change the program" from a default into a last resort.
For Fitness Enthusiast Eric: next time you catch yourself debating a new split or a new coach, run the audit on yourself first. Sleep, protein, energy availability. If any of those three is not at threshold, the new program will not save you.
We earlier ranked the variables INSIDE the program in The 80/20 of Training Results; this post ranks them OUTSIDE. Together they form a complete diagnostic loop: before-you-change-the-program / after-the-program-is-dialed-in. Bookmark both. For the comprehensive nutrition science underpinning the seven variables, the Evidence-Based Nutrition & Recovery Guide is the pillar reference. FitFlow's client tracking system makes the seven lifestyle variables visible across your entire roster, so the Off-Program Audit becomes an automated dashboard instead of a manual pass.
Download The Off-Program Audit — Run It Before You Change the Program. 20 questions across 7 lifestyle domains. Ranked intervention plan per client. 5 refer-out guardrails for the boundary cases (REDS-S high-risk, mental health, sleep disorders, CKD, disordered eating). 4-week intervention templates per variable. Print one per client; run at every check-in. Download the Free Audit.
Frequently Asked Questions
Comments