What the 2026 Hydration Research Actually Shows — And Why Your Certification Taught You the 2007 Version

Most trainers still teach scheduled fluid intake every 15–20 minutes. NATA 2025 and the current research say that's the right call for some clients — and the wrong call, possibly a dangerous one, for most.
Educational content for fitness professionals. Not medical advice. Consult a physician, sports dietitian, or other qualified healthcare provider before changing a client's hydration or nutrition program — especially for clients with cardiovascular, renal, or endocrine conditions.
The Client Walks In With an LMNT Packet
A client shows up to a 7am summer session holding an LMNT sachet. "I saw Huberman talking about this. Should I crush it before we train, or after?" You give the answer you've been giving — stay ahead of dehydration, electrolytes are a good idea in the heat. The client nods, mixes it, trains, leaves.
You've just transmitted ACSM 2007. The research moved on roughly a decade ago. NATA's 2025 fluid-replacement position statement formalized the shift (NATA, 2025). Most trainer certifications haven't caught up because most curricula refresh on a 5–8 year lag.
This post is the catch-up. It synthesizes three things the 2026 evidence has materially changed — when to drink, how much sodium, and who is actually at risk — and rebuilds them into a protocol you can use this week.
The contrarian frame upfront: the bigger hydration risk for most of your general-population clients isn't dehydration. It's over-drinking hypotonic fluid. And the smaller subset of clients who genuinely need electrolytes are systematically buying products that are undersodiumed for the loads they're sweating. The $44.9B consumer market is engineered around the wrong customer (Coherent Market Insights, 2026). Your job is to flip the equation for the people you train.
If you're still defaulting to "drink 8 oz every 15 minutes," your certification is teaching the 2007 protocol. Get the 2026 protocol.
Why This Topic Became Urgent in 2026
Three time-stamped anchors push this from evergreen reference into this-month urgency. Men's Journal, Feb 2026 named LMNT "Best Electrolyte Powder for Athletes 2026" after a sweat-test evaluation. US News Health, Feb 28, 2026 ran "Electrolyte Supplements Are Everywhere. Who Benefits From Them and When?" — mainstream press framing the practitioner question on a national stage. And the global electrolyte drinks market hit $44.9B in 2026, growing at 5.9% CAGR toward $63.4B by 2033 (Coherent Market Insights, 2026) — an alternative Fortune Business Insights estimate puts it at $43.1B with an 8.4% CAGR. Either way: more product velocity, more client questions per session.
The knowledge-gap math is just as concrete. Most working trainers were certified under ACSM 2007 guidance, embedded in NASM and ACE curricula. NATA 2025 has materially updated the standard (NATA, 2025). The trainer who synthesizes this for clients owns the trust transfer that follows.
For the broader nutritional context, see .
The Three Things That Changed
Three evidence-backed corrections. Each framed the same way — old guidance, current evidence, what it means for client work.
Change 1 — The Drink-to-Thirst Debate Has a Resolution (for Most Sessions)
Old guidance (ACSM 2007): drink ahead of thirst; schedule fluid every 15–20 minutes during exercise.
Current evidence (2026): for sessions under 90 minutes at moderate intensity in cool-to-moderate conditions, thirst-driven intake is safe and effective. Hew-Butler et al.'s 2018 narrative review in Journal of Athletic Training (PMC5790864) synthesized the planned-versus-thirst literature and found no demonstrated performance impairment or dehydration risk from moderate body-mass loss in those conditions. A 2025 Nutrients review of ultra-endurance hydration extended the finding into longer durations, with caveats around heat and individual sweat rate.
Two design caveats worth naming. The foundational evidence is largely observational and field-based, not RCTs with hard endpoints. And "drink ahead of thirst" was itself a response to documented voluntary hypohydration in uneducated recreational athletes — a real but specific population. For coached clients taught to recognize signals, that concern is reduced.
Scheduled intake remains right in three contexts: sessions over 90 minutes, exercise in heat or humidity, and athletes with documented high sweat rates. Outside those, the default flips.
The primary risk of mandatory scheduled hydration is overconsumption of hypotonic fluids — the leading mechanism for exercise-associated hyponatremia (EAH). Even the Gatorade Sports Science Institute's own review acknowledges the trade-off, which is notable given GSSI is product-adjacent.
What this changes in your client work: replace "drink every 15 minutes" with a tiered protocol based on session length, intensity, and environment. Teach thirst plus urine color as primary signals for everyday training. This is also one of .
Change 2 — Sodium Needs Vary by Roughly a Factor of 15
Old guidance: "Have a sports drink during exercise to replace electrolytes." Generic, dose-blind.
Current evidence (2026): sodium loss in sweat varies from roughly 200 mg to over 3,000 mg per liter — about a 15-fold range between individuals (NATA, 2025; JISSN 2018 individualization studies). The range is wider than the difference between any two consumer products on the shelf.
NFL, NBA, and Olympic programs use individualized sweat testing because a universal protocol leaves some athletes chronically under-replaced and others over-supplemented. NATA 2025's explicit recommendation is individualized hydration plans based on measured sweat rate, sport dynamics, and environmental factors. That is the standard of care — not yet the standard of practice in commercial gyms, which is the opening.
The product-shelf problem: most consumer electrolyte products contain 100–400 mg of sodium per serving. For a high-sweat-rate athlete losing 1,500–3,000 mg Na/L, this is systemically under-replacing. Even LMNT — the highest-sodium mainstream product at ~1,000 mg per serving (drinklmnt.com) — can fall short during heat training.
Target range, consistent with NATA guidance: 500–900 mg Na per liter of fluid for moderate-to-high-sweat athletes; 900–1,500 mg/L for salty sweaters; little to none for low-sweat clients training indoors under 60 minutes.
The contrarian claim, plain: most consumer electrolyte products are undersodiumed for the clients who actually need them. And most clients who buy them don't need them at all. Your role is to help clients figure out which category they're in — which requires a sweat rate estimate, not a brand opinion. For complex cases, refer to a registered dietitian nutritionist (RDN) or sports dietitian.
Change 3 — Over-Drinking Is a Real Risk, Not Just an Ultramarathon Problem
Old guidance: EAH only happens to ultramarathoners. General fitness clients should err toward drinking more.
Current evidence (2026): EAH is serum sodium below 135 mmol/L during or within 24 hours of activity (NIH StatPearls NBK572128). Severe EAH (<120 mmol/L) causes CNS symptoms from cerebral edema; fatal cases documented at <110–115 mmol/L. The mechanism is excessive hypotonic fluid in excess of sweat losses.
The "only ultrarunners" framing is outdated. A 2019 Hew-Butler narrative review (PMC6780610) documents EAH across multiple sport types, including recreational athletes during hot-weather exercise. Recent 2025 EAH literature reinforced the Wilderness Medical Society 2019 prevention framework.
Hold the incidence numbers two ways: symptomatic EAH at marathon-distance runs is typically under 1% per event — which sounds small until you multiply. With 55,000+ NYC Marathon finishers in 2025, even a sub-1% rate is hundreds of symptomatic cases per single event. Most are mild and self-resolve. A subset is not. Limitation worth flagging: prevalence in non-elite general training populations remains under-studied — the current literature explicitly calls this out.
The dangerous part is symptom overlap with heat illness. Nausea, headache, confusion, and bloating present in both. Treating EAH as heat illness and administering more fluid worsens it.
What this changes in your client work: any client with nausea, headache, or bloating during or after a session — especially in heat, especially with reported high plain-water intake — should not automatically receive more fluid. The corrective for suspected EAH is sodium-containing fluid and medical assessment for severe cases. Recognition is within trainer scope. Diagnosis is not — refer out for evaluation.
Teaching clients to drink as much as possible isn't wrong because it fails for dehydration. It's wrong because it can directly cause a separate medical condition that dehydration does not.
The Hydration Prescription Protocol
The practitioner tool no competitor in the trainer editorial space provides. Three steps. A scale. Four minutes per assessment.
Step 1: Estimate Sweat Rate (Field Method)
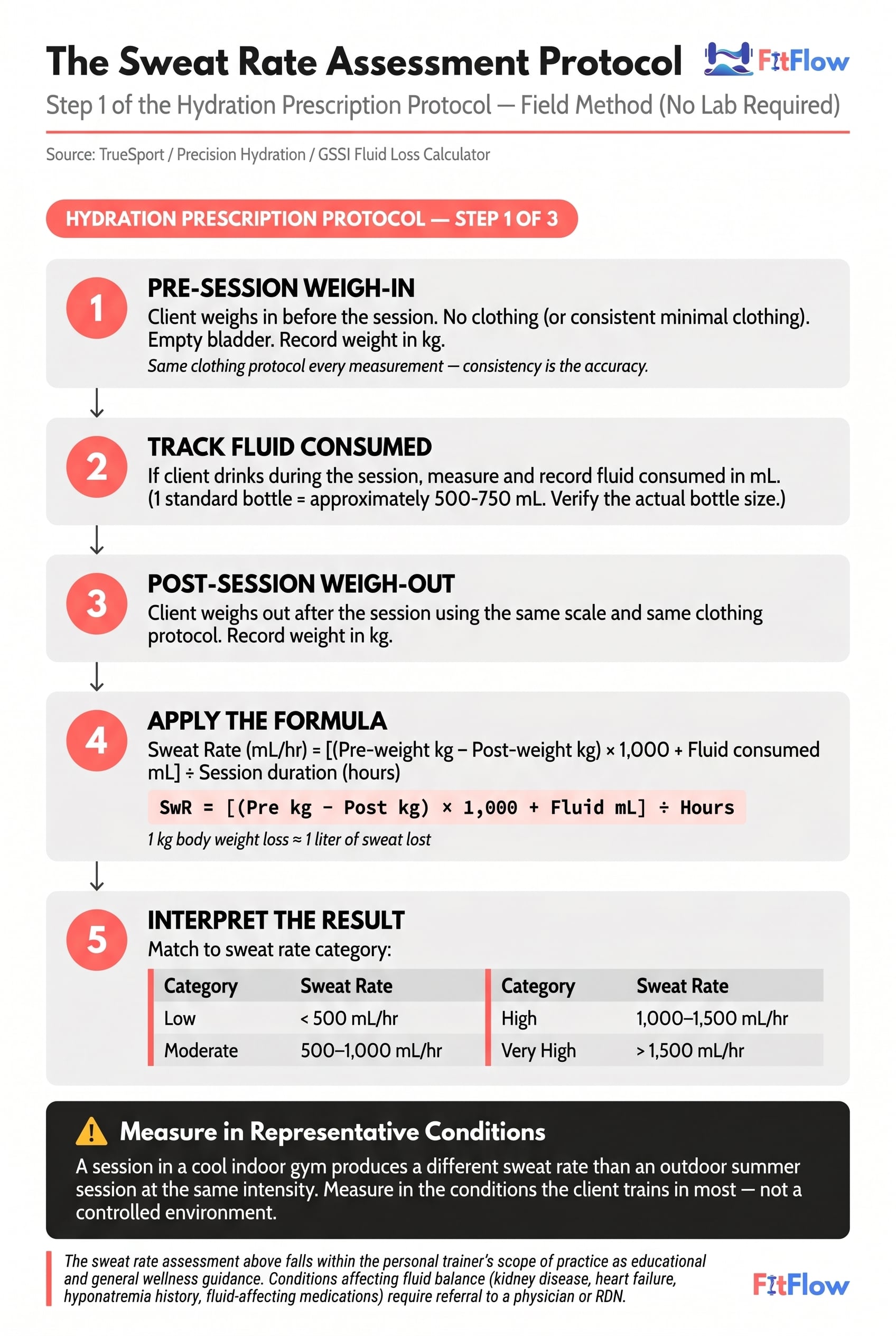
The pre/post-session body weight method, refined by Precision Hydration and the GSSI Fluid Loss Calculator:
Client weighs in pre-session — minimal consistent clothing, empty bladder.
Client doesn't drink during the session (or tracks fluid consumed in mL).
Client weighs out post-session in the same clothing.
Sweat rate (mL/hr) = [(Pre-weight kg − Post-weight kg) × 1,000 + Fluid mL] ÷ Session duration (hours).
1 kg body weight loss ≈ 1 L sweat.
Category | Sweat Rate |
|---|---|
Low | <500 mL/hr |
Moderate | 500–1,000 mL/hr |
High | 1,000–1,500 mL/hr |
Very High | >1,500 mL/hr |
Measure in representative conditions. A cool-gym indoor assessment won't predict an August outdoor 10K. Source: TrueSport sweat-rate methodology; Precision Hydration field protocol.
Step 2: Identify Sodium Loss Category (Field Proxy)
Lab patch testing is the clinical gold standard. Most trainers won't have access. Field proxies are approximations, not diagnoses — use them to triage, not to prescribe with precision.
Low (~<500 mg Na/L): little visible salt residue; no strong salty sweat taste; no cramp history.
Moderate (~500–1,000 mg Na/L): some visible salt lines on dark clothing; mild salty taste; occasional cramping in heat.
High / "salty sweater" (~>1,000 mg Na/L): heavy white salt residue; strong salty taste; frequent cramping during long or hot sessions; fatigue or headache after sessions even when subjectively hydrated.
Framework consistent with Today's Dietitian and Precision Hydration sweat-sodium methodology.
Step 3: Sodium Replacement Tier Selection
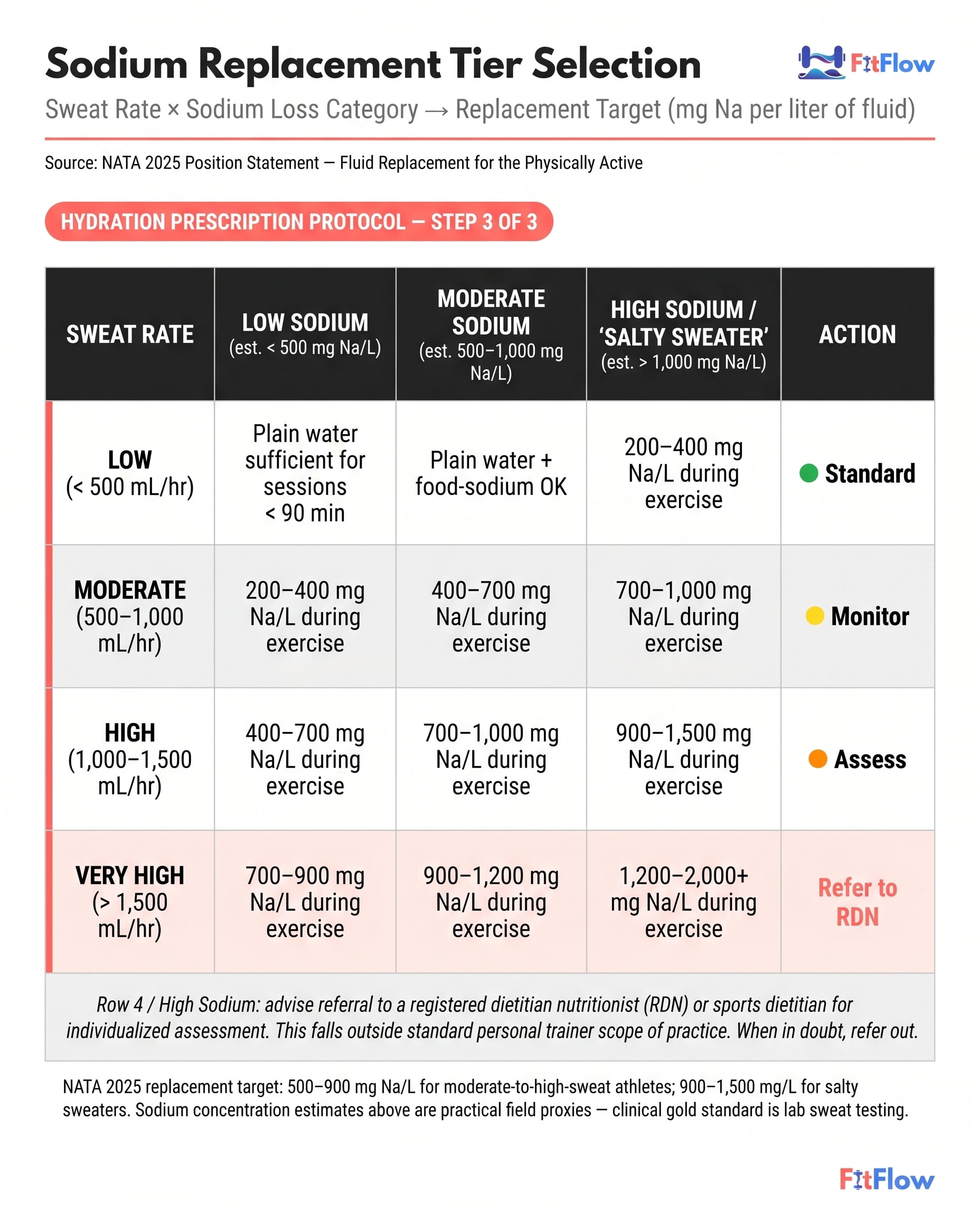
Combine sweat rate × sodium category for a replacement target per liter of fluid consumed during exercise:
Sweat Rate | Low Sodium | Moderate Sodium | High Sodium |
|---|---|---|---|
Low | Plain water <90 min | Water + food-sodium OK | 200–400 mg Na/L |
Moderate | 200–400 mg Na/L | 400–700 mg Na/L | 700–1,000 mg Na/L |
High | 400–700 mg Na/L | 700–1,000 mg Na/L | 900–1,500 mg Na/L |
Very High | 700–900 mg Na/L | 900–1,200 mg Na/L | 1,200–2,000+ mg Na/L — refer to RDN |
The protocol above is the framework. The calculator does the prescription. Get the calculator (free).
Scope of practice: sweat rate assessment and the ranges above sit inside the personal trainer scope as educational and general wellness guidance. As a trainer, you support client decisions — you don't prescribe medical treatment. Specific medical conditions affecting fluid balance — kidney disease, heart failure, hyponatremia history, medications affecting sodium handling — require physician or RDN referral. Hypertensive clients should consult their physician before increasing sodium intake. When in doubt, refer out.
Hydration prescription integrates cleanly into .
The Product Landscape — Evidence-Based Filter
The $44.9B market gives clients a lot of shelf options. The decision collapses to one organizing variable: sodium content per serving.
What to look for: (1) Sodium 500–1,000 mg per serving for genuinely high-sweat athletes; most consumer products land at 100–400 mg. (2) Potassium and magnesium support muscle function but are secondary — and the magnesium-for-cramps marketing claim runs ahead of the controlled-trial evidence in exercise contexts. Observational support is decent. RCT support is limited. (3) Sugar is a fuel decision, not a hydration decision — useful for sessions over 60–90 minutes at high intensity, unnecessary for shorter sessions. (4) Simple ingredient list. Adaptogens, B vitamins, and collagen aren't doing the hydration job.
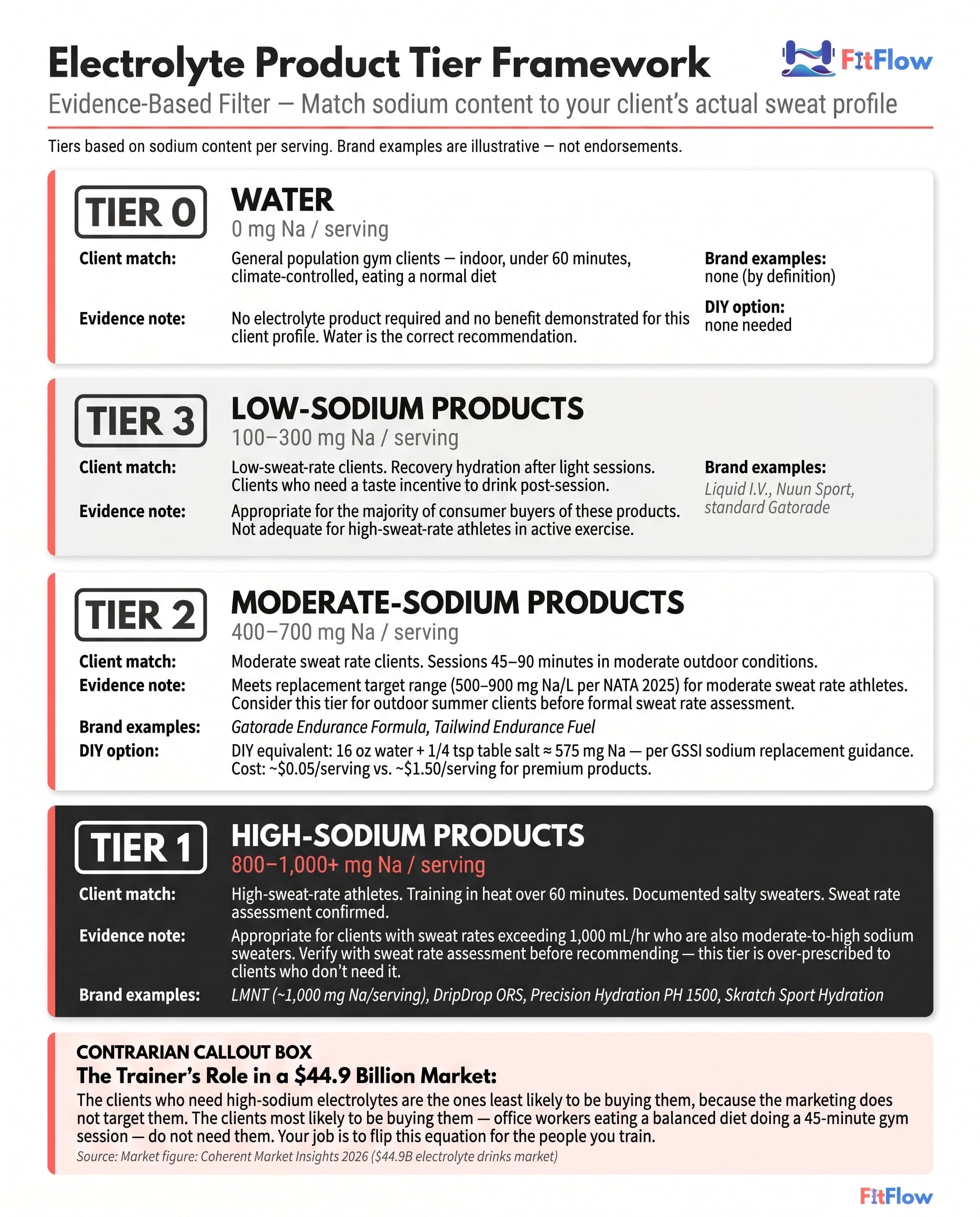
Product category tiers (brand-neutral; brands named only as tier examples, not endorsements):
Tier 1 (800–1,000+ mg Na/serving): high-sweat athletes, heat training >60 min, salty sweaters. Examples: LMNT, DripDrop ORS, Precision Hydration PH 1500, Skratch Sport Hydration.
Tier 2 (400–700 mg Na/serving): moderate sweat, 45–90 min in moderate conditions. Examples: Gatorade Endurance Formula, Tailwind Endurance Fuel.
Tier 3 (100–300 mg Na/serving): Examples: Liquid I.V., Nuun Sport, standard Gatorade. Recovery hydration or low-sweat clients who need palatability incentive to drink.
Tier 0 (water): the majority of general-population clients training <60 min in cool-to-moderate conditions. No electrolyte product needed; no benefit demonstrated.
Disclosure: Brand names above are listed as tier exemplars for educational purposes. FitFlow has no affiliate relationship with the products named. Tier placement is based on publicly listed sodium content per serving as of May 2026. Formulations change — verify the label.
The contrarian summary: the clients who need high-sodium electrolytes are least likely to be buying them. The clients most likely to be buying them — office workers eating a balanced diet doing a 45-minute strength session — don't need them. Your job is to flip this equation.
DIY option: 16 oz water + ¼ tsp table salt (≈575 mg Na) + citrus + a small amount of honey ≈ Tier 2 at ~$0.05/serving versus ~$1.50/serving for premium products. Consistent with GSSI sodium replacement guidance. Pair it with .
How This Applies by Client Type
Type A: General Population Gym Client
3–5 sessions per week, strength or mixed training, climate-controlled gym, 45–60 min. Sweat rate likely Low to Moderate. Support strategy: plain water before and during; post-session electrolytes only if the client skips meals or eats very low sodium. Common error: recommending a product because the client saw it on social media. That creates a $40 per month dependency habit with no measurable benefit. NEAT and overall daily activity affect baseline hydration needs more than any sachet — see .
Type B: Summer Outdoor Athlete
Running, cycling, outdoor group fitness; 60–120 min in heat and humidity. Sweat rate likely Moderate to High. Support strategy: 16 oz water 2 hours pre-session. Drink to thirst during. If the session exceeds 90 min or heat index tops 90°F, transition to scheduled intake (7–10 oz / 15–20 min) with a Tier 2–3 product. Post-session: 16–24 oz per pound of body weight lost if measured. Heat acclimation note: clients training through summer naturally heat-acclimatize over 7–14 days. Sweat rate increases. Sweat sodium concentration decreases as aldosterone-driven sodium conservation improves. Reassess sweat rate at week 1 and week 3. The spring baseline under-predicts July sweat volume.
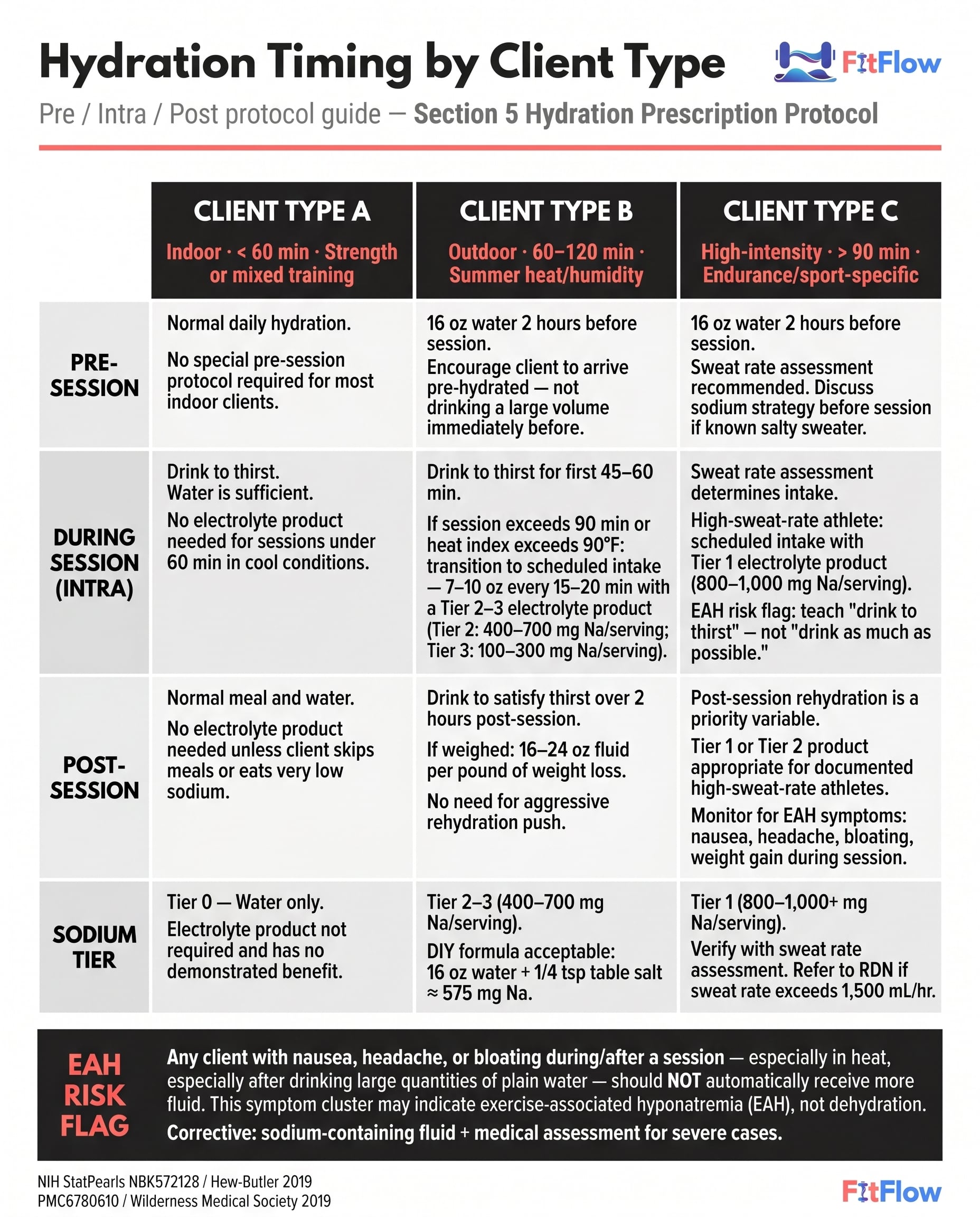
Type C: High-Intensity / Long-Duration Athlete
Marathon, triathlon, competitive sport, HIIT >90 min, heat sessions. Sweat rate likely High to Very High. Support strategy: a formal sweat rate assessment is warranted. Sodium replacement is a performance and safety variable. Refer to an RDN or sports dietitian if sweat rate exceeds 1,500 mL/hr or the client reports persistent cramping, nausea, or extreme fatigue despite standard hydration. A Tier 1 product (800–1,000+ mg Na/serving) is likely appropriate — verify with the assessment first. EAH flag: this client has the highest EAH exposure. Educate explicitly on "drink to thirst" rather than "drink as much as possible." Weight gain during a long heat session is a hard indicator of over-drinking and warrants stopping fluid intake and medical evaluation if symptomatic.
Hydration Markers and the Caffeine Myth
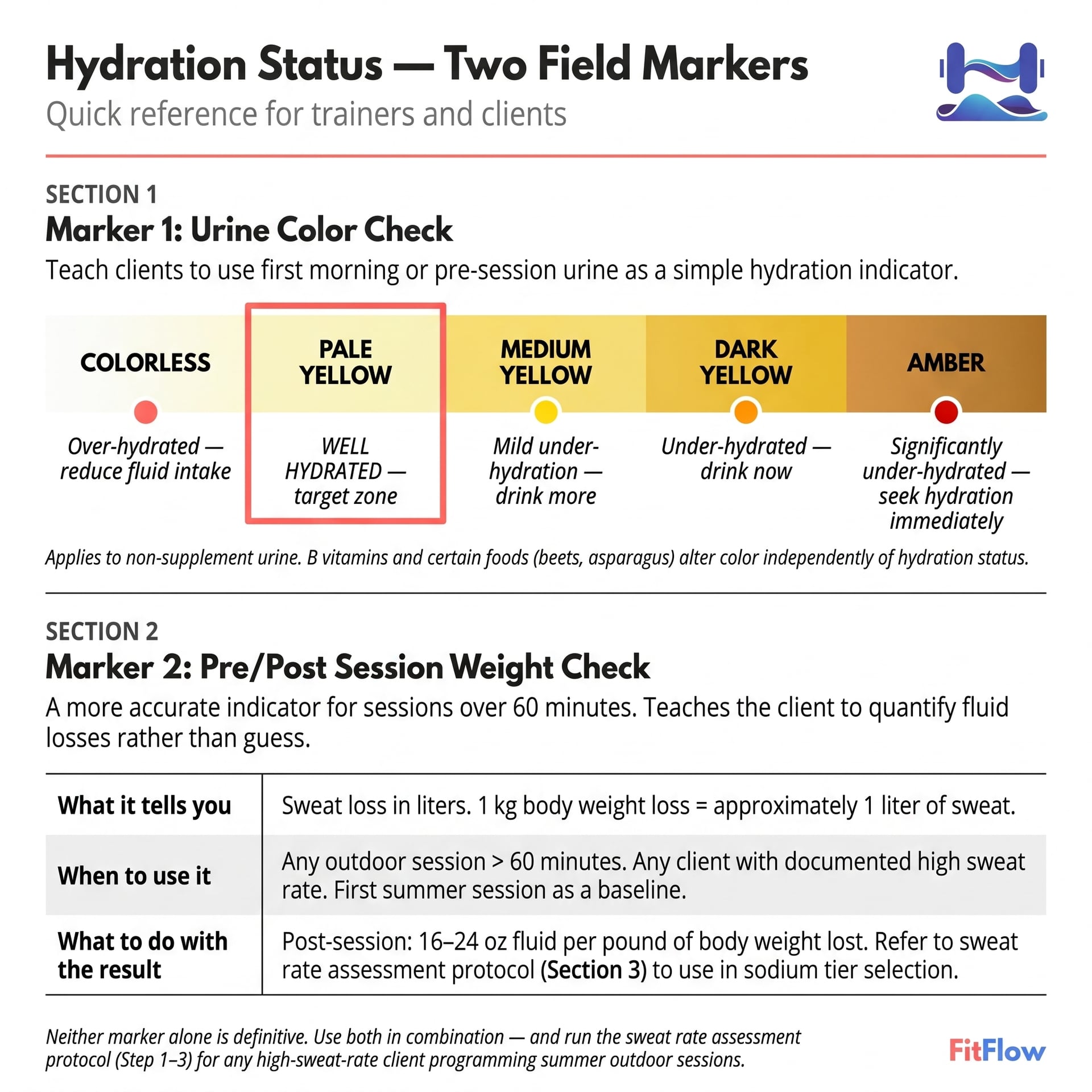
For everyday client assessment, three markers in combination beat any single number — the WUT framework (Weight, Urine, Thirst):
Urine color: pale yellow = well hydrated; dark = under; colorless = potentially over. Caveat: riboflavin (B2) tints urine yellow independent of hydration.
First-morning body weight: stable within ±1% suggests stable hydration. A 2%+ overnight drop suggests under-replacement from the prior session.
Thirst: lags real need in untrained populations. It is a reliable real-time signal in coached, educated clients for sessions <90 min. The signal-quality difference is exactly why trainer education shifts the protocol default.
Serum sodium and urine specific gravity are clinical measurements. If a client presents with persistent symptoms despite a reasonable protocol, refer them out.
On daily baseline vs. pre-training: daily total water for sedentary-to-lightly-active adults is roughly 30–35 mL/kg/day, sourced from beverages and food (food contributes 20–30%). The "drink half your bodyweight in ounces" formula is a folk heuristic with no peer-reviewed basis. It lands in the right ballpark for a 70 kg adult and miscalibrates at the extremes. Pre-training top-up is separate: 16 oz water 2 hours before sessions of 60+ minutes, especially in heat.
Does caffeine cause dehydration? Durable myth, worth correcting. Moderate caffeine (up to roughly 400 mg per day for most healthy adults — pregnant and breastfeeding clients should consult a physician) does not produce a meaningful net diuretic effect in habituated users during or after exercise. The ISSN position stand on caffeine and exercise performance reaches the same conclusion (Guest et al., 2021, JISSN). The original "coffee dehydrates you" claim came from short-term studies in caffeine-naive subjects at high doses. Stop telling clients to drink extra water to "offset" their coffee.
The Summer 2026 Trainer Protocol Checklist
Assess: identify duration category (<60 / 60–90 / >90 min). Identify environment (indoor / outdoor moderate / outdoor heat). Ask about cramping history. Ask about post-session nausea, headache, or bloating (EAH flag). Run a sweat rate assessment for any client training >60 min outdoors in summer.
Support the client's decision: indoor <60 min → water to thirst, no product. Outdoor 60–90 min moderate heat → water to thirst; Tier 2–3 if salty-sweater signs. Outdoor >90 min, heat >80°F → scheduled intake (7–10 oz / 15–20 min); Tier 2 minimum. High-sweat athlete outdoors → Tier 1 product; formal assessment. Very High sweat (>1,500 mL/hr) → RDN referral.
Educate: teach urine color (WUT model). Teach pre/post weight check for any summer outdoor session >90 min. Correct the "drink as much as possible" myth. Provide tier guidance matched to sweat profile, not brand marketing. Schedule a Q4 hydration check-in for any client on a summer protocol.
What This Means Going Forward
The 2026 evidence didn't invent new physiology. It clarified individualization. The pre-2010 era treated all athletes as a single dosing population because the alternative was operationally expensive. Sweat-patch testing, wearable hydration biosensors, and field-method protocols have lowered that cost to the point where individualization is cheap — sometimes free, when the only tool is a digital scale you already own.
The trainers who internalize this will be the practitioners clients trust when the next consumer product wave arrives. (And it will arrive — wearable sweat sensors, continuous hydration monitoring, and AI-driven intake suggestions are already moving from elite-sport pilots toward consumer release; industry tracking flags this as the next 24–36 month frontier.) The trainer with a defensible sweat-rate protocol and a sodium-tier framework absorbs those tools without disruption. The trainer still teaching the 2007 schedule is re-learning the basics under client pressure.
Two things to do this week. First, run the sweat-rate protocol on yourself. Calibrate the tool on your own body before bringing it to a client. Second, pick one current Type B summer outdoor athlete and run the full three-step Hydration Prescription Protocol with them. The whole conversation takes one session. The credibility transfer lasts months.
Get the calculator that automates the math. The Hydration Prescription Calculator takes session duration, environment, estimated sweat rate, and salty-sweater flag, and returns a sodium tier recommendation, a product criteria checklist, and a ready-to-share client protocol in under 60 seconds. It includes the printable Sweat Rate Assessment Worksheet and an EAH symptom-recognition quick reference. Brand-neutral. Trainer-facing. Free.
Inline sources: NATA 2025 Fluid Replacement Position Statement (nata.org/sites/default/files/2025-08/fluid_replacement_for_the_physically_active.pdf); Hew-Butler et al. 2018 (PMC5790864); MDPI Nutrients 2025 ultra-endurance review; NIH StatPearls EAH (NBK572128); Hew-Butler 2019 (PMC6780610); Wilderness Medical Society 2019 EAH guidelines; Gatorade Sports Science Institute; Coherent Market Insights 2026; Fortune Business Insights 2026; Today's Dietitian; Precision Hydration; TrueSport; LMNT product specifications (drinklmnt.com/pages/ingredients); US News Health (Feb 28, 2026); Men's Journal (Feb 2026); ISSN position stand on caffeine and exercise performance (Guest et al., 2021, JISSN). Last reviewed: 2026-05-17.
Editorial disclosure: FitFlow has no affiliate or commercial relationship with any electrolyte brand named in this article. Product names are listed as tier examples based on publicly available sodium-per-serving data as of May 2026. Verify product labels before recommending — formulations change.
Frequently Asked Questions
Comments